Lyme disease (LD) is a vector-borne illness caused by the spirochete Borrelia burgdorferi and transmitted in the United States by blacklegged ticks (Ixodes spp.).
LD is most commonly found in the northeastern, mid-Atlantic, and north-central regions of the United States (1).
In 2005, New Jersey reported 38.6 LD cases per 100,000 population, the third-highest incidence in the United States after Delaware and Connecticut (1).
Since 1980, New Jersey has mandated that health-care providers and clinical laboratories report all LD cases to local health departments, which investigate these reports to confirm that they meet the national surveillance case definition.
Reports from health-care providers typically include exposure and clinical information needed for case confirmation.
In contrast, reports from laboratories do not contain exposure and clinical information, and local health departments must follow up with health-care providers to obtain the missing information needed to confirm a case for surveillance purposes.
In 2002, New Jersey expanded its paper-based laboratory reporting system to include electronic laboratory-reporting (ELR) for all laboratory-reportable diseases.
During the next 4 years, New Jersey's local health departments noted that the number of ELR reports for LD and the time needed to handle them had begun to impede the departments' abilities to address other public health priorities.
In 2006, to assess these concerns, the New Jersey Department of Health and Senior Services evaluated the state's LD surveillance system.
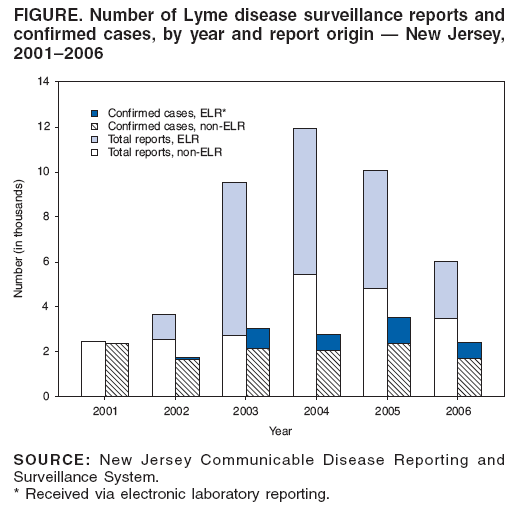
This report summarizes the results of that evaluation, which determined that during 2001--2004, the total annual number of LD reports increased nearly fivefold (from 2,460 in 2001 to 11,957 in 2004), but confirmed reports increased only 18% (from 2,371 in 2001 to 2,791 in 2004).
ELR represented 51% of reports received during 2001--2006, but only 29% were confirmed upon investigation.
These results illustrate the difficulties associated with ELR reporting of LD in New Jersey, especially the use of resources needed to address other public health problems.
Other states with similar difficulties might need to reevaluate the resources used to confirm electronically reported LD and other notifiable diseases.
CDC guidelines for surveillance system evaluations were used to conduct the evaluation (2).
Key LD surveillance parameters (e.g., total number of LD reports, number of confirmed LD cases, origin of reports [i.e., ELR versus non-ELR], and investigation completion status) during 2001--2006 were obtained from the New Jersey Communicable Disease Reporting and Surveillance System (NJCDRSS).
NJCDRSS was implemented in 2001, and surveillance data from before 2001 are limited to the number of confirmed LD cases per year.
For surveillance purposes, NJCDRSS used the national case definition for LD, in which a reportable case of LD was defined as
1) physician-diagnosed erythema migrans greater than 5 cm in diameter or 2) one or more objective late manifestations of LD* with laboratory evidence of infection with B. burgdorferi (i.e., isolation of the organism or positive serologic testing) in a person with possible exposure to infected ticks (3).
Reports with laboratory evidence of infection alone were not considered to be cases. The surveillance case definition remained constant throughout this period.
By using NJCDRSS data and chi-square analysis, the geographic, age, and seasonal distribution of ELR reports was compared with that of non-ELR reports.
NJCDRSS data did not permit differentiation of paper-based reports from paper-based health-care provider reports within the surveillance database; therefore, both types were included in the non-ELR category, and analysis of ELR reports compared with non-ELR laboratory reports was not possible.
Surveillance system personnel were interviewed to obtain information regarding investigation processes, surveillance system structure and flow, funding, and personnel resources.
Total annual LD report volume increased from 2,460 in 2001 (before introduction of ELR) to a peak of 11,957 in 2004 before decreasing to 6,015 in 2006 (Figure).
From the introduction of ELR in 2002 through 2006, electronic reporting accounted for a substantial number of annual LD reports, ranging from a low of 1,142 (in 2002) to a high of 6,799 (in 2003).
These ELR reports accounted for 31%--71% of total annual reports but only 5%--33% of confirmed cases per year (Figure).
The absolute number of confirmed cases during 2001--2006 remained steady.
Among the 13,567 confirmed cases reported during 2002--2006, ELR and non-ELR cases differed significantly by patient residence (p less than 0.05) and time of year that illness onset occurred (p less than 0.05).
Proportionately more confirmed non-ELR cases (8,067 of 9,958; 81%) than confirmed ELR cases (2,350 of 3,609; 65%) were associated with residence in the higher LD-prevalence region of northern New Jersey than with southern New Jersey.
A higher proportion of confirmed non-ELR cases had onset dates during the usual LD transmission season of April--September (6,999 of 8,465; 83%) than confirmed ELR cases (2,191 of 3,031; 72%).�
ELR and non-ELR confirmed cases did not differ by patient age (median: 42 years for both).
For the period 2001--2006, LD investigations required a median of 2 months to complete follow-up and classify the report (range: less than 1 week--8 months), representing approximately 1 hour of active information collection per case.
The balance of the 2-month period was time spent waiting for health-care providers to respond to information requests.
Diversion of investigators to other public health priorities also caused delays in LD investigations.
Approximately 24% of investigations during the period 2001--2006 were not completed before the close of each surveillance period and were not included in the year-end final surveillance case numbers.
Reports that were confirmed after the close of the surveillance period were updated in NJCDRSS for the preceding year but were not included in the published surveillance data.
State surveillance system personnel reported that before the introduction of ELR, a substantial but unmeasured proportion of paper-based laboratory reports was never entered into the electronic database that served as the "investigation pending" list because of a limited number of data-entry personnel.
With the introduction of ELR in 2002, all incoming electronic reports were placed automatically on this list.
The effect of this change was to substantially enlarge this list and to place a greater demand on local health department personnel as they attempted to process the greater number of pending reports.
As a result, personnel diverted attention from other public health duties.
In 2004, the year when the total number of reports referred for investigation peaked, the time required for LD report follow-up peaked at 11,957 hours (or approximately 5.75 full-time--equivalent� investigators) statewide, compared with 2,460 hours in 2001, before the advent of ELR.
Reported by: LA McHugh, MPH, S Semple, MS, FE Sorhage, VMD, CG Tan, MD, New Jersey Dept of Health and Senior Svcs. AJ Langer, DVM, EIS Officer, CDC.
Editorial Note:
Because of this investigation, New Jersey is modifying its LD surveillance system to reduce the surveillance burden (i.e., the cost of conducting LD surveillance in terms of personnel committed and funding required).
New Jersey has adopted the revised national LD surveillance case definition (Box) (4), implemented in January 2008, which provides local and state health departments with additional flexibility to classify LD reports as confirmed, probable, or suspect cases.
Although the revised national surveillance case definition alone likely will not decrease the LD surveillance burden in New Jersey or other states, it will provide a more complete measure of the surveillance burden and guide development of sustainable surveillance systems that are consistent among states.
After New Jersey's introduction of ELR in 2002, the subsequent increase in LD reports referred for investigation likely reflected technological improvements in data acquisition and not an actual increase in the number of laboratory reports received.
After ELR initiation, the additional volume of pending laboratory reports exceeded local investigative capacity.
Although the available capacity for local investigations was not calculated as part of this evaluation, the inability of local health departments to complete LD investigations in a timely manner likely indicates that available resources in New Jersey were inadequate to meet the demand for these investigations.
Previous reports have illustrated the complexity of LD surveillance in the United States (1,5).
In New Jersey, ELR implementation increased the proportion of total laboratory reports that were referred for investigation; however, the annual total number of confirmed cases remained steady.
Whether the steady number of confirmed cases during 2001--2006 is an actual reflection of the incidence of LD in New Jersey or merely reflects the maximum number of reports that could be confirmed given available resources is unknown.
The causes for the observed decrease in LD reports during 2005--2006 have not yet been established.
This analysis revealed statistically significant differences, by both county and season, between confirmed LD cases in terms of report origin (i.e., ELR versus non-ELR).
These differences likely were caused by greater use of paper-based health-care provider (non-ELR) reports during the warmer months, when ticks are more active.
This pattern likely is attributable to a higher proportion of patients with early-stage LD caused by recent infection, for which serologic testing typically is not necessary for diagnosis.
In addition, in the northern region of the state, where LD prevalence is higher, health-care providers might be more likely to clinically diagnose (and subsequently report) LD.
Laboratory reports are useful to identify LD cases that otherwise might not have been reported by health-care providers and are an important component of LD surveillance in New Jersey.
The findings in this report are subject to at least three limitations.
First, LD surveillance is influenced by several factors not examined in this evaluation (e.g., accuracy of laboratory tests for LD and willingness of health-care providers to report early-stage cases); accordingly, not all potential determinants of LD surveillance burden are considered in this report (1,5).
Second, demographic and clinical data for all confirmed LD cases were not available, and additional differences might exist between cases detected by ELR versus non-ELR beyond those described in this report.
Finally, analysis of ELR versus non-ELR laboratory reports was not possible, which prevented comparison of laboratory-reporting types independent of the possible influence of paper-based health-care provider reports.
To address the problems identified in this report, in January 2008, New Jersey began automatically classifying all new ELR LD laboratory reports that meet laboratory evidence criteria� as suspected cases under the new surveillance case definition (4).
To reduce the burden associated with contacting health-care providers, investigators will only follow up on laboratory reports if a concurrent report is received from a health-care provider, until planned enhancements to NJCDRSS are in place that will permit automated mailing of case-report forms to health-care providers for patients with positive LD laboratory test results.
Some laboratory reports not accompanied by a paper-based health-care provider report also will be investigated on a case-by-case basis.
This change is expected to reduce the burden of follow-up on LD reports.
New Jersey will continue to evaluate and refine its LD surveillance system to reduce surveillance burden while improving the quality of surveillance data.
2. CDC. Updated guidelines for evaluating public health surveillance systems: recommendations from the guidelines working group. MMWR 2001;50(No. RR-13).
3. CDC. Case definitions for infectious conditions under public health surveillance. MMWR 1997;46(No. RR-10).
6. CDC. Recommendations for test performance and interpretation from the Second National Conference on Serologic Diagnosis of Lyme Disease. MMWR 1995;44:590--1.
7. Dressler F, Whalen JA, Reinhardt BN, Steere AC. Western blotting in the serodiagnosis of Lyme disease. J Infect Dis 1993;167:392--400.
8. Engstrom SM, Shoop E, Johnson RC. Immunoblot interpretation criteria for serodiagnosis of early Lyme disease. J Clin Microbiol 1995;33:419--27.
9. CDC. Caution regarding testing for Lyme disease. MMWR 2005;54:125.
* For purposes of surveillance, late manifestations include any of the following when an alternative explanation is not found:
1) recurrent, brief attacks (during a period of weeks or months) of objective joint swelling in one or a few joints, occasionally followed by chronic arthritis;
5) encephalomyelitis (confirmed by a higher titer of antibody against B. burgdorferi in the cerebrospinal fluid than in serum); or
6) acute onset of second- or third-degree atrioventricular conduction defects that resolve in days to weeks and are occasionally associated with myocarditis.
� Differences in denominators for geographic and temporal analyses are the result of missing data.
� 2,080 hours per year.
� For purposes of surveillance, laboratory evidence of infection with B. burgdorferi is defined as a positive culture for B. burgdorferi, two-tier testing interpreted using established criteria, or single-tier immunoglobulin G immunoblot seropositivity interpreted using established criteria (6--9).
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services.References to non-CDC sites on the Internet are provided as a service to MMWR readers and do not constitute or imply endorsement of these organizations or their programs by CDC or the U.S. Department of Health and Human Services. CDC is not responsible for the content of pages found at these sites. URL addresses listed in MMWR were current as of the date of publication.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
-------------------- Note: I'm NOT a medical professional. The information I share is from my own personal research and experience. Please do not construe anything I share as medical advice, which should only be obtained from a licensed medical practitioner. Posts: 4881 | From Middlesex County, NJ | Registered: Jul 2006
| IP: Logged |
Maybe all the states should be MORE passive about their reports and just accept them, rather than going thru all kinds of gyrations to exclude them. The lab report says positive, then it is positive and it counts. I suspect that all these investigations are only to reduce the number of reported cases and that is how it will work out. But then they find it takes too much time so then they look for ways to reduce cases and take no health dept time. Result: no lyme cases reported at all or a farcical number.
I remember hearing years ago about a huge forest fire outside Moscow, made the sky glow orange at night, cinders falling in the city streets. There was no mention of any fire in the newspapers or other media. Has our govt been learning tricks from the Russians?
Posts: 8430 | From Not available | Registered: Oct 2000
| IP: Logged |
bettyg
Unregistered
posted
thx for posting and for BREAKING it up for folks like me!!
IP: Logged |
The Lyme Disease Network is a non-profit organization funded by individual donations. If you would like to support the Network and the LymeNet system of Web services, please send your donations to:
The
Lyme Disease Network of New Jersey 907 Pebble Creek Court,
Pennington,
NJ08534USA http://www.lymenet.org/









 UBBFriend: Email this page to someone!
UBBFriend: Email this page to someone!




![[Wink]](wink.gif)
![[hi]](graemlins/hi.gif) )
)

![[group hug]](graemlins/grouphug.gif)
![[kiss]](graemlins/kissing.gif)




 Printer-friendly view of this topic
Printer-friendly view of this topic