TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
quote:Originally posted by bluelyme: Has any one done rife through microscopy to verify frequency kills or has anyone done before after of killer agents?
bluelyme,
I tried watching under the scope while I used a Beam Ray rife machine early last year, but I couldn't see much response with the frequencies I used. That machine never did a whole lot for my borrelia that I could tell. It seemed to help with other infections and symptom relief when it helped.
Then again, I didn't have the energy to pursue it more than a few times. I honestly would have liked to have subjected my slides to a different machine such as a BCX. You need a "broadcast" machine to even try this experiment. A contact machine will not work. But, a Doug Coil would. It would be interesting to try it with a Doug Coil, actually. I don't know of anyone who has one, though.
I KNOW rife works! I just don't have the equipment to do more experiments at this point. I am using a borrowed contact device at the moment.
Have you seen Anthony Holland's youtube videos on shattering cancer with frequencies? He uses a plasma tube. I hear that he has also done successful experiments with borrelia, but has done that work "underground." He claims it takes a machine that can run at least two frequencies simultaneously, with the 2nd frequency being the 11th harmonic of the base frequency.
As for herbal agent microscopy experiments, "Wakeup" proposed that back in August of last year on this thread. It's page 4 (8-11-2015). See my response in the very next post.
Maybe you could put a bug in Wakeup's ear for her to get a microscope and to get started doing her own experiments. I would like to contribute, but mostly it is just too labor-intensive for me to do controlled "studies." Besides, I am on ABX and can't discontinue them at this point.
[ 01-30-2016, 09:20 PM: Message edited by: TNT ]
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
posted
Does anyone have any good references for/describing artifact visible in dark field?
As well as any examples/references for normal structures found in the blood that would possibly resembler spirochetes?
I am just trying to make sure that the structures I am seeing are indeed spirochetes, and not normal, benign structures like fibrin strands, etc.
I can't find any decent examples, or references to look at. It seems that very little exists for dark field microscopy, in this realm.
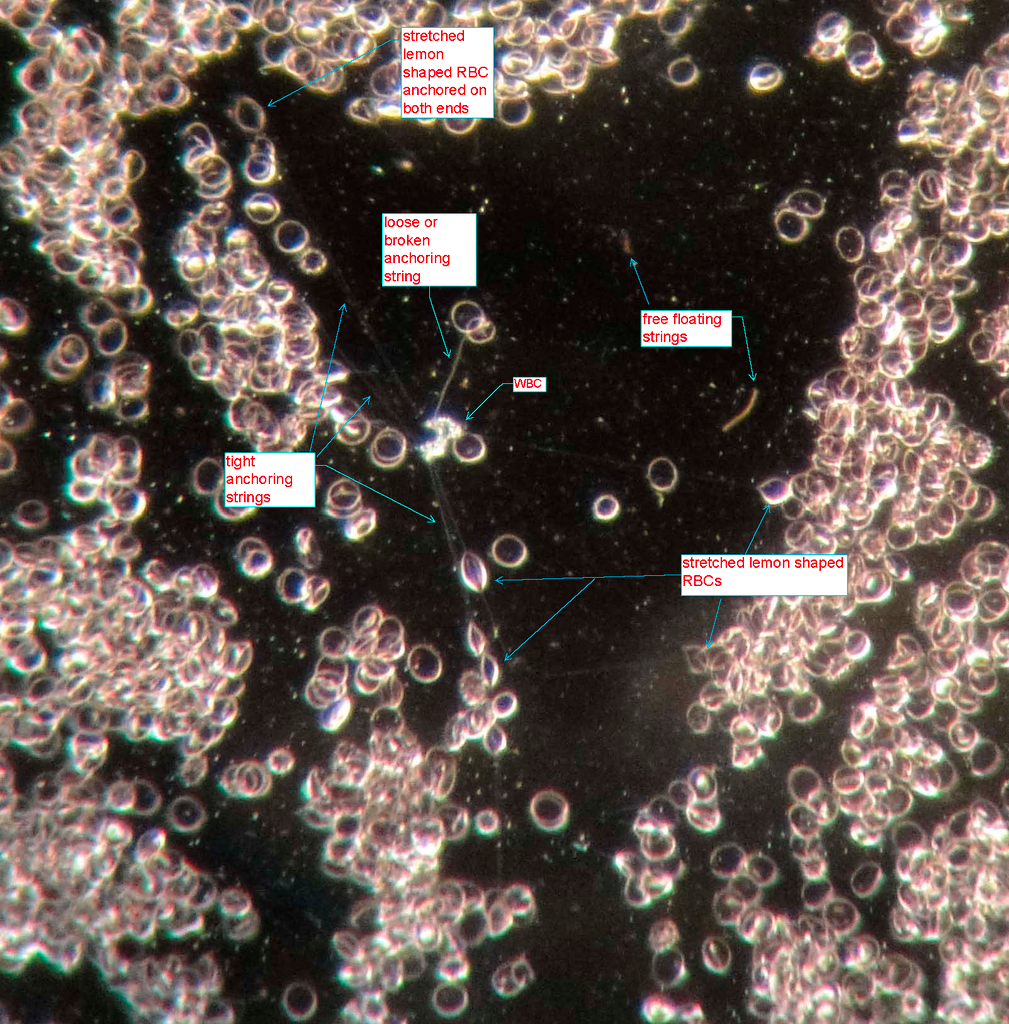
For example, what would be found within erythrocytes, that are long strands, that could possibly anchor them to a slide? See below image, above the yellow dots.
What can't be seen in the photo is the fact that these structures are anchoring the RBC's in place. They don't appear to be different in nature to the other spirochetal structures in my samples, when not anchored to the slide. The RBC is still freely moving within the serum, but this structure anchors it.
It is debatable whether or not borrelia can be intracellular, especially in RBC's. But I so often see these structures either coming out of RBC's, anchoring them to the slide, etc. What normal component would do this, and have this appearance?
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
I don't know of any dark-field references off hand.
But, I really think that those connecting strings are fibrin. They are not undulating are they? Take your last video for instance. It was not attached to anything and it was undulating...and moving freely in the plasma.
But, I know what you mean. Even though we feel certain about what we are seeing, we want verification from a reputable reference.
Morten Laane's work may give you a clue. Other than that, ...???
Great job, by the way! Your 1000x darkfield is working out wonderfully!
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
Anecdote: Significant increase in spirochete/spirochete like structures compared to fresh/non-incubated sample viewed immediately after blood draw. Purely subjective estimation of 4-5 fold increase in visible spirochetes.
Samples are drawn into syringe. One slide is immediately prepped with a sample for viewing prior to injection into Vacutainer for storage/incubation. New samples produced daily for viewing. Best time frame I've noted for viewing samples is 72 hours after draw/incubation. ~94 degrees fahrenheit for incubation is based off both personal, subjective experience as well as referenced from other studies conducted stating that temperature range is optimal for long term culture. (Caveat: Those studies used culture medium. I do not. Those studies were long term, months long cultures. I "culture" for up to 5 days before discarding samples). I call these spirochetal/spirochete like structures because I am not a trained pathologist, nor do I have any capability to definitively determine that these structures are indeed bacteria.
Take a look!
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
Here, this article talks about the issue of pseudo-spirochetes, particularly when conducting live blood analysis/dark field microscopy.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
Sample: 3.0ml Whole Blood, 7.0 mL EDTA Vacutainer Sample prepped immediately after draw (from vacutainer, didn't plan on doing initial slide sample tonight, but decided to and immediately drew from the vacutainer, so the sample is not fresh in the sense that it has been reconstituted with EDTA from the container) Video is 4 hrs after slide prep
Relevant info: Control sample Patient has no known illness/disease/infection
Anecdote: Control samples, for my purposes, are simply samples drawn from individuals with no known, diagnosed, or suspected illness/disease/infection. Samples are treated in the same way as "infected" samples. Draw of the sample, slide preparation and viewing, storage of the sample in EDTA, and incubation times for further slide preparations are the exact same. Note lack of structures/organisms that are spirochetal in nature. Continuation of slide viewing at 12 hours, in the morning, along with further slide preparations at varying stages from the incubated sample will also provide more pictures/video.
I've got lots of video, and need to create an organized video presentation of them.
Also, to note, my equipment used. Amscope T490B-DK Equipped with 100X OIL objective with adjustable iris Canon 70D DSLR (with DSLR adapter for view through the trinocular port on top of the microscope)
The 70D provides great video and photo, as it is 18.4? megapixels, but even with software update, I don't think it is capable of doing time lapse photography in a single file (it will do time lapse, but each new image is a separate file, which I don't want to deal with combining).
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
posted
I am curious how others feel about a few things regarding this work.
Many resources I look at reference the length of time it takes to culture Borrelia, and specialized culture mediums. I have read a few references, including the Mattman resources linked here and elsewhere, the discuss the intracellular nature of Borrelia.
So, a few things to consider: 1) The increase in these organisms/structures with simple incubation of samples: Are these truly spirochetes growing in this environment? Is it artifact? An phenomenon produced from the break down of components of the blood sample (strands of protein, etc). Is it a combination?
2) Comparison to known and suspected samples. The "spirochetes" visible in these samples look like the non-motile (or whatever your preferred term is) form of the spirochete from examples of uncultured Borrelia. Are they the same? Examples of artifact? I am still looking for definitive examples of any debris that could possibly mimic the shape, etc.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
Current treatments: Tinidazole 500mg bid, Minocycline 100mg bid
Anecdote: Significant increase in spirochete/spirochete like structures compared to fresh/non-incubated sample viewed immediately after blood draw. Purely subjective estimation of 4-5 fold increase in visible spirochetes.
Samples are drawn into syringe. One slide is immediately prepped with a sample for viewing prior to injection into Vacutainer for storage/incubation.
So, it appears that this video was made with a sample that was fresh, that was NOT subjected to the Vacutainer beforehand, and viewed immediately. Blood was from chronically ill person (you) who was concurrently on treatment (of special note is the Tinidazole-a known cyst-killing ABX).
Contrary to your next video in which sample was immediately made using fresh blood- FROM Vacutainer-, but not viewed until 4 hours later. Blood was from an otherwise healthy person who was not on ABX.
I personally feel that those "spirochetes" in the video of YOUR blood are INDEED true spirochetes!
What I notice in the second sample (from healthy individual) are what appear to me to be cysts. Particularly, I notice them at :30, :35, and :40. -- (https://www.youtube.com/watch?v=IYTLWXWSmrA&feature=youtu.be)
My thoughts on the "healthy" person's blood:
Could there have been conversion in the "healthy" blood because of the EDTA in the Vacutainer? Or, was the immune system strong enough to keep the ketes dormant in the cystic form regardless of the EDTA?
It would be interesting to see a sample from the same "healthy" individual not subjected to EDTA (Vacutainer) and viewed immediately.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
posted
Yea, I should have viewed the blood right away. I injected the blood into the EDTA vacutainer, then decided to do a slide anyways. So the sample was fresh, as it just drawn, but had already been exposed to the EDTA.
However, I didn't notice anything in the control sample. I should note, also, that I did view it immediately. The "4 hours later" is actually when the video was taken. No change between the immediate view and when the video was taken.
Most of what you see is normal artifact, cellular debris and normal components of blood. There is also expected artifact from the use of EDTA. With future slide preparations, I will consider the sample to be a clean, negative control in the absence of spirochetal structures.
I am also trying to get my hands on some BSK. Anyone know where to get any? (Sigma Aldrich only sells to registered research laboratories).
As an interesting side project, I am very likely to make my own. The components, and amounts used to create it, are available online. And even though I can't purchase the medium, it is possible to purchase each individual component. I'm about to set up my own high school science experiment.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
Dr. Bela Bozsik shows us video of Borrelia spirochetes in human blood at the NorVect conferences in 2014. This is the same exact thing that most of us see in our Lyme Diseased blood!!!!!
The NorVect conferences are the most reputable of gatherings that everyone in the whose who of Lyme Disease research & treatment goes to. The information shared by top doctors & researches (Dr. Alan MacDonald, Dr. Richard Horowitz, Dr. Eva Sapi,...etc) these presentations are considered very valuable.
Posts: 2094 | From NY | Registered: Oct 2011
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
posted
One of the biggest new optical microscopy technology companies has put out videos stating that these dancing strings are spirochetes (Borrelia burgdorferi) in human blood, but the CDC can't?
From the video: " This video illustrates spirochetes (Borrelia burgdorferi) associated with Lyme Disease in a live red blood cell culture. This video was captured using a research grade optical microscope equipped with CytoViva's patented enhanced darkfield optical illumination system." https://www.youtube.com/watch?v=XWR7AFcgKSc
Then I contacted CytoViva & asked about how those videos were obtained & their confidence that it was Borrelia b. & this is what they had to say.
"Thank you for your interest in CytoViva technology and the ability to observe Borrelia and related organisms. Our patented enhanced darkfield microscopy enables the capture very high signal-to-noise images of these types of pathogens in-situ in tissue, blood cells and other environments.
By adding hyperspectral imaging to the microscope, you can spectrally characterize these pathogens in these different environments.
The video you referenced was captured by microbiology researchers at Auburn University who were studying Borrelia. These bacteria were specifically cultured by this microbiology group.
CytoViva provides fully equipped optical microscopes for this type of imaging and can also provide integrated hyperspectral imaging as required.
Please let us know how we can support you with more insight regarding this technology. "
Posts: 2094 | From NY | Registered: Oct 2011
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
quote:Originally posted by thatdudefromkansas: Most of what you see is normal artifact, cellular debris and normal components of blood. There is also expected artifact from the use of EDTA. With future slide preparations, I will consider the sample to be a clean, negative control in the absence of spirochetal structures.
Have you looked at any of your (own blood) samples over the long-term? Most of us are finding granules (in the absence of spirochetes) in the samples of older blood in which initially there were numerous spirochetes. In my experience, week-old blood has many granules and no spirochetes.
I think that until you can positively identify what the artifacts are you cannot prove that what you are seeing are not Borrelia morphologies.
What I am saying is that it is impossible to know that a sample does NOT contain Borrelia without the use of DNA typing/staining in the absence of typical Borrelia spirochetal structures.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
posted
"What I am saying is that it is impossible to know that a sample does NOT contain Borrelia without the use of DNA typing/staining in the absence of typical Borrelia spirochetal structures. "
True, I always dismiss everything bleb or cyst like, unless I see many bulbous tip spirochetes or SOP in the area.
Look at this wbc time lapse as when it lyses it can produce cyst & bleb like objects, which is the same thing I have witnessed & tried to describe in my video. At times though the wbc's do carry borrelia cysts & they can uncoil to show the spirochetes atypical structure. I see the cysts burst out when I do hot baths & check my blood after 1 hr as I mentioned before.
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
quote:Originally posted by thatdudefromkansas: I am curious how others feel about a few things regarding this work.
thatdudefromkansas,
I hope you don't regard my comments in the above posts as negative criticism, because I think you are doing awesome work, and approaching this very scientifically. Keep up the good work, and good luck in making your own BSK medium. We would be very interested in the details. I might try it myself if not too expensive.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
However, criticism is always a good thing if the purpose is constructive. If something is wrong, point it out.
Science cannot progress with criticism.
I think it is always best to approach this problem with two mindsets. The current one that you are correct, and these are spirochetes. The other being critical, that these are not, and actively pursuing any reason why these would not be spirochetes.
So I am also actively pursuing references or resources to the contrary of my beliefs. To cover both sides.
What was interesting, if you read that document I presented about "pseudo-spirochetes" is that they noted the difference between the true spirochetes and the pseudo-spirochetes thusly: Transmission electron micrograph of a pseudospiro- chete, showing dark homogeneous protoplasm, as is typical of eryth- rocytes, and lack of both an outer envelope and endoflagella. Pseu- dospirochetes appear in and out of the plane of focus because of their irregularly curved morphology Reference: http://vdi.sagepub.com/content/3/4/350.full.pdf
But there are both naturally occurring as well as laboratory modified mutants of borrelia that lack flagella, and as a consequence, also have altered morphology.
Altered motility and morphology of mutant SC-E1.Analysis of targeted mutations in the major flagellin gene, flaB, indicated that loss of PFs in B. burgdorferi influences both cell morphology and motility (46, 59). Because the hook is essential for flagellum assembly in other bacteria, we determined if the cell morphology and motility of SC-E1 were also altered. Dark-field microscopy revealed that whereas wild-type spirochetes had a flat-wave morphology, SC-E1 cells were rod shaped and often grew in chains (Fig. 1a and b). Moreover, electron microscopic examination of thin sections of SC-E1 revealed that the cells completely lacked PFs (Fig. 1c and d). These observations further support the conclusions, drawn from analysis of the flaB mutant, that the PFs influence the shape of cells and have a pronounced skeletal function (46). We also tested whether the motility of SC-E1 was altered. Dark-field microscopy examination of SC-E1 indicated that the cells were completely nonmotile. Furthermore, in contrast to the wild-type cells, SC-E1 cells did not swarm on swarm agar plates (Fig. 1e and f). These results indicate that SC-E1 resembles the previously characterized flaB mutant (46, 59); both strains were deficient in filament synthesis, were rod shaped, and were nonmotile. Reference: http://jb.asm.org/content/190/6/1912.full Photomicrographs of mutants described in this work
So it is possible, as well, that the identification of a spirochete like structure as a "pseudo-spirochete" based on the lack of endoflagella/periplasmic flagella (PF) or a variation in the protoplasmic cylinder is potentially flawed as well. I will look up more resources tonight regarding protoplasm of Borrelia. What variations can occur naturally, in mutants or normal Borrelia? Would that cause the appearance to be like described above, in the pseudo-spirochete?
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
posted
Also, if anyone is interested, I might be willing to part with a Darkfield Condenser.
.7-.9 NA Dry. I have the OIL one I use exclusively now, so the condenser that came with my T490 is not being used.
Good for 40x magnification. Some of the images I have shared have been 40x, but with a 20X eyepiece.
As long as you have a standard microscope, it should fit perfectly fine.
So, with the purchase of a set of 20x eyepieces, you could get relatively decent magnification/resolution at 800x.
If anyone is curious or interested, let me know. It doesn't mean anyone that borrows it will get to keep it for the long run, but I am willing to loan it out for any period of time.
I'm wlling to share =)
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
posted
thatdudefromkansas and others thank you for all your links and info. I often find thicker free floating strings only in areas with lots of RBCs anchored by thin strings, which suggests, that the thicker free floating strings were created from broken anchoring strings. Lots of times I find several stretched lemon shaped RBCs anchored in circular pattern around shrinking bubble or single WBC like in picture below. All free floating strings I find are dead. They are just punched around by Brownian motion. At certain point they disintegrate in to tiny pieces. I have seen one floating string disintegrate in just few minutes. I don’t think that the free floating strings are spirochetes.
I think figuring out how to incubate borrelia from blood sample might be the only chance to somehow see it and verify that it still exists in some type of form. I found some instructions on how to do it here: http://www.medsci.org/v10p0362.htm Culture media can be possibly purchased here? http://www.sigmaaldrich.com/catalog/product/sigma/b8291?lang=en®ion=US I noticed that in 15th minute of video https://www.youtube.com/watch?v=WozrCFW0mRM Lida Mattman points out that they just grow borrelia directly on slides inside of coplin staining jar. How? I don’t know. It’s possibly tricky. I estimate that coplin staining jar could be partially submerged in bucket of water with cheap self regulating aquarium heater and hold same temperature as expensive incubator. If somebody figures it out please let us know. I will start trying when I’m off of abx.
[ 02-06-2016, 04:13 PM: Message edited by: Sobre ]
Posts: 8 | From USA | Registered: Feb 2016
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
Sobre, welcome to Lymenet, and to this thread!
That's an interesting picture. I have personally never seen those "strings" that you and dude have shown. Nor have I seen the lemon-shaped RBCs. It's kind of odd because I've looked at a lot of blood. I'm not sure what the difference may be that you guys are seeing this and I'm not.
Do you have video footage of that same spot the picture was taken? I would be interested in seeing how those components were moving.
Please tell us about your lyme journey and fill us in on your microscope equipment!
Thanks for joining!
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
The strings anchoring the RBC's in place didn't appear to be fibrin, as fibrin is often readily visible on my slides as well, and there is a stark difference in the way fibrin appears. I figured it was some mechanism I didn't fully grasp that was causing that kind of cellular debris that might mimic an atypical spirochete. Also explains the limited presence of these structures in the blood of non-infected individuals.
A good question beyond this is, how long do these structures last? And what is a distinguishable difference between those and an atypical spirochete that would have a similar shape.
Also, it is quite hard to differentiate between anything living and dead to the brownian motion, as you have stated.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
posted
TNT the video is here http://vid411.photobucket.com/albums/pp198/sobre3/1_zpsqgrsky7p.mp4 It’s not really good one. I only have 400x dark field and hand held camera. I use AmScope T690C. It uses infinity objectives and AmScope doesn’t sell 100x infinity objective with adjustable iris to match their dark field condenser. I think I will try AmScope 60x infinity objective or try to get lucky on Ebay with some other brand 100x objective. Can somebody recommend time-lapse camera setup?
The video shows 24 hour old sample left at room temperature. I’ve been doing this only for few weeks and haven’t witnessed how WBCs manage to get tangled in RBC strings while creating small clearing in carpet of RBCs. That slide had about 5 similar spots on it while other slides may not have anything or just couple of spots. Possibly preparation of slide might have something to do with it. The slide with 5 spots was from drop of blood so small that it didn’t need to be smeared and edges of drop started to coagulate little bit before I covered it. On some slides I have seen RBCs getting stretched by strings around air bubble and once also next to channel of flowing RBCs when blood kept flowing on slide for extended period of time. Since yesterday I goggled it and only found few live blood analysis pictures with lemon shaped RBCs pointing to protein linkage, which has something to do with digestion of proteins and only sounds like theory.
My Lyme has been rash half year ago, then month and half of trying to figure out what it is, after that standard doxy, after that other classic Lyme symptoms and now mixtures of abx for few months.
Posts: 8 | From USA | Registered: Feb 2016
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
Thanks Sobre! That video was helpful.
The only real way to definitively determine if those strings are ketes (besides culturing) is to do the borrelia stain with fluorescence like Dr. Alan MacDonald and Peter Kemp are doing. Though, I would be hesitant to conclude that those "detached strings" are not spirochetes. They may just be devitalized, or more dormant than wild-type. Take a look back at some of the criteria that we (particularly Lymedin2010) have given for spirochetes.
I definitely appreciate your work and contribution! That nature.com article was interesting and very helpful. I had never heard of apoptosis creating beads-on-a-string before. It's possible that, at least some of what we are seeing, is apoptosis. As dude has reminded us, we need to maintain an open mind and approach this objectively.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
Sobre, are you seeing things that you could confidently call spirochetes?
Also, could you view a sample over a week's time, and then report what you find (you will have to seal off your coverslip to keep the sample from drying out)? I know I have found spirochetes at first, then fewer and fewer until no spirochetes, but more and more granules til the end of the week.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
posted
PeterKemp, if you are still active here.....
I'm looking to expand my experimentation with microscopy and culturing, as well as any tests I could competently perform.
You seem to have some personal experience in doing this yourself.
Any ability to point me in the right direction or help me out with the processes you have used to conduct your own research?
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
posted
Peter does not come here anymore, but he listed all his materials & methods on his website. He got the idea of using sodium citrate from Morten Laane & his paper.
Months into his experiment the atypical & flat strands grew into more typical spiraling spirochetes.
QUOTE: "Materials and methods The medium to hold blood cells stable on a microscope slide mini-culture was prepared as: Deionised water with:- Sodium Chloride 9 gms/litre Sodium Citrate 3 gms/litre Dextrose 5 gms/litre Triton X-405 0.5 mls/litre Gelatine granules were dissolved in the liquid as per the manufacturer's instructions (Dr Oetker Gelatine - www.oetker.co.uk) to create a soft jelly. The slide was prepared as a normal blood drop thin-film smear on a Polysine TM (Thermo Scientific) cell adhesion microscope slide. No drying time was allowed. A drop of the prepared medium was immediately placed on the smear and a 50mm coverslip placed. After blotting, the periphery of the coverslip was sealed with microscope immersion oil."
Posts: 2094 | From NY | Registered: Oct 2011
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
posted
You can use this to grow spirochete, as it also contains a bit of sugar as well.
-0.65g per 100ml of RODI or Distilled water -Add 1 drop of solution above to 1 drop of your blood directly on the slide. -Try this with a completely sealed slide (use Vaseline if doing 40x) & try with all sides sealed except leave one side open. This is because Bb will be depending on proper O2 vs CO2 to encourage to grow.
Posts: 2094 | From NY | Registered: Oct 2011
| IP: Logged |
posted
Interesting, might have to look into something like that.
As a side note:
In the absence of any manufactured culture medium, I've been thinking of other culture methods. Then it dawned on me----- Why not do a skin biopsy, and use that tissue for a substitute medium. Biopsy a sample, divide it, and then culture a number of ways: One culture in whole blood, one culture in plasma, one culture in whole blood diluted with something like glycerol, etc etc. However, essentially crush/grind the skin sample so that, in the culture, it can be stirred prior to drawing for creating a slide.
My thinking was that the next best medium might be host tissue. A skin biopsy is a simple thing if I can get a kit.
I'm also looking into creating, or getting as near to creating, my own BSK medium. That's not to say that it will have all the ingredients. If the best I can do is a medium lacking an ingredient, I'll take that.....better than nothing, and still might yield results greater than simply incubating whole blood.
What do y'all think?
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
quote:Originally posted by thatdudefromkansas: I'm also looking into creating, or getting as near to creating, my own BSK medium. That's not to say that it will have all the ingredients. If the best I can do is a medium lacking an ingredient, I'll take that.....better than nothing, and still might yield results greater than simply incubating whole blood.
What do y'all think?
Sounds like a plan! I would also give Lymedin2010's suggestions a try. They sound simple enough.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
posted
Do you have Lyme Disease think skin & red rashes? I know I do & culturing from there is on my list. I predict that if we are carrying as many spirochetes, blebs & cysts as we carry in our blood, then we are shedding some in our skin in general & should be able to culture them from skin shavings/slothing.
They used microscopy & culturing way before any PCR or the new DNA sequencing was available. Willy Burgdorferi was able to find spirochetes in blood, CSF & skin well before 1984 using microscopy, yet somehow this concept eludes the CDC. All of a sudden in the 21st century where technological advances inundates us we become moronic to such concepts.
"This suggestion was strongly supported by the subsequent isolation of seemingly identical spirochetes from the blood (3, 12), cerebrospinal fluid (12), and skin (12) of patients acutely ill with Lyme disease and the further demonstration of immunological reactivity of patient sera with the spirochetes (12). "
" The cells are gram negative and stain well with Giemsa and Warthin-Starry stains. Unstained cells are not visible by bright-field microscopy but are visible by dark-field or phase-contrast microscopy. "
"A review of reports on the genetic and phenotypic characteristics of strains of the spirochete which causes Lyme disease revealed that these organisms are representative of a new species of Borrelia. We propose the name Borrelia burgdorferi for this species. The type strain of B. burgdorferi is strain B31 ( ATCC 35210). "
posted
The reason for culturing with skin biopsy is also to use it as a medium for growth.
The intent would be the introduction of the biopsied tissue into a sample of some component of infected blood. That would be cultured.
A control would be a second biopsy, or simply dividing the single biopsy tissue into multiple parts, and culturing that in the same conditions, but in the absence of infected blood.
It would simply provide a haven, with nutrients, that might yield better results than just blood.
It's just an idea I was thinking about, and am looking into other sources to see what has already been done with this method, and seeing what results were reported.
The BSK medium is rich in nutrients that borrelia needs which is why it yields such good results. But, host skin tissue also has nutrients ideal for borrelia. So it might be a culture medium of compromise, in lieu of being able to get my hands on BSK.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
posted
TNT Everything on my slides seems to start degrading after 24 hours. (I have been sealing all 4 sides so far.) For example the area where I took posted picture had only couple of tight strings left following day and eventually they all disappeared. I have seen floating string disintegrate in to granules, but I would not be able to distinguish the granules from all other debris. I see more and more debris with time but that’s everywhere and it appears to come mostly from decomposing white cells. There are only few strings in just few areas of slice so they can’t create too much debris.
[ 02-09-2016, 03:56 AM: Message edited by: Sobre ]
Posts: 8 | From USA | Registered: Feb 2016
| IP: Logged |
posted
Thank you guys, you are wealth of information. I’m trying to come up with some logic on how to use microscope as tool to monitor results of treatment but I’m not sure I understand everything correctly. It appears that there are following ways to detect borrelia body parts which can still multiply or reproduce:
1) Grow corkscrewing spirochetes Advantage is that it’s 100% accurate (if successful) Disadvantages are 5 month delay and complexity of process. It’s also not very useful if you know you are infected and only want to compare counts of bacteria to some other sample.
2) Use antibody stain to detect stained strings I think this one should be also 100% accurate as any strings in blood samples appear to disintegrate in matter of days. If fresh string managed to assemble itself from components which get stained by borrelia antibody I would bet that same components can also multiply or assemble something than can further multiply.
3) Use antibody stain to detect stained anything (blobs, etc.) Possibly not 100% accurate as even components which can no longer multiply might get stained.
4) Use other stains than antibody stain. I don’t know much about this one, but I think this type of stain might also stain other stuff. If stained strings show up, that might be interesting.
5) Look for any string in blood. Advantage is that it’s very simple and almost instant but not 100% accurate. However if string can be found with same characteristics and behavior as string found by antibody stain that could significantly increase accuracy. I guess it all depends on antibody staining technique. If there is antibody staining technique which doesn’t damage RBCs and even keeps strings attached to RBCs that would be great.
If you can please let me know if you see any errors in this or if you have additional ideas on it. Thank you
[ 02-09-2016, 04:11 AM: Message edited by: Sobre ]
Posts: 8 | From USA | Registered: Feb 2016
| IP: Logged |
posted
Dude I noticed in link from Lymed on this page http://counsellingme.com/microscopy/bskculture.html line: “various quantities of BSK 2 (with 6% rabbit serum) have been used from 2 to 10mls (it has been suggested by an expert that bovine serum might be better)” Bovine serum appears to be sold by more places than BSK so I was thinking that it might be easier to buy. Also around 37th minute of video https://www.youtube.com/watch?v=WozrCFW0mRM MPM media is mentioned. Instructions on how to make it appears to be here. http://lymerick.net/MPM-2001-medium-Bb.html It however looks like ingredients for it may also not be easy to get plus it’s tricky to use.
Posts: 8 | From USA | Registered: Feb 2016
| IP: Logged |
The quote about bovine serum being better is as a preparation material for the BSK. So, not Bovine serum alone, but with BSK and bovine serum as opposed to BSK with rabbit serum.
MPM media might be interesting to experiment with, but I read another study stating that the MPM media doesn't actually work. Wouldn't stop me from trying it, though.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
posted
OK, it looks like there is a problem with my theory on antibody stain: Fluorescent microscope for couple thousand $ is needed.
Posts: 8 | From USA | Registered: Feb 2016
| IP: Logged |
posted
Yes, fluorescent microscopy can have a very high startup cost.
Cheap filter system, maybe 1500 dollars, plus stains..... So, if you really, really like doing this, and you can afford to sell your left nut, then got for it, haha.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
bluelyme
Frequent Contributor (1K+ posts)
Member # 47170
posted
If you guys can test cultures and their suceptability to antimicrobials and find one that works in vivo i will volunteer an appendage or two...
-------------------- Blue Posts: 1539 | From southwest | Registered: Dec 2015
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
posted
Peter Kemp has suggested dioralyte & says it alone can grow spiros, but still a bit tricky as some have still not been able to grow it even with BSKII added yet.
I think mine has grown & sometimes hard to tell from the many spiros exiting rbc's & have to do controls. I messed up the first rounds with too much Vaseline on the cover slip & it mucked up the slides.
Rabbit serum + dioralyte is another method & really you can use any serum. You can even get human serum & put it in a container with a hole & boil it. You can have this on the cheap & do this before you spend any money. Even going to a farm butchering shop & asking for rabbit or any animal blood for real cheap, boil + dioralyte, and then adding 1 drop of this to 1 drop of your blood on the slide.
Try with part of slide unsealed, as you need ratio of O2 to CO2 to be just right & try with sealed too.
Posts: 2094 | From NY | Registered: Oct 2011
| IP: Logged |
posted
OK my theory form post above on using fluorescent antibody stain to verify if floating strings are borrelia L-forms has another problem: Borrelia L-forms in form of string apparently can not be stained by FITC antibody stain. Message at 1 minute 45 seconds in this video https://www.youtube.com/watch?v=rqbWWTslbLM points it out. Plus there are no picture of stained strings before they turn to spirals anywhere.
Posts: 8 | From USA | Registered: Feb 2016
| IP: Logged |
posted
Lymed, I ordered it. Do you think that if successful the dioralyte might generate visibly increased number of floating strings in a matter of days and that would indicate possibility of being on right track to grow spinning spiral forms in few months?
Posts: 8 | From USA | Registered: Feb 2016
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
posted
Yes. You may have to leave 1 side open at least & seal the rest. I would try seal all & another slide leave one side.
I think Niall Cronely might be Peter Kemp, it sure looks like his work. Maybe what we are seeing in our blood are very stagnant & slow growing Bb & as a result they do not produce large quantities of antibodies on their surfaces & as a result do not stain well. Or perhaps what little proteins they generated were shed.
Persister cells are also known to grow very slow & have a very low metabolic rate. This is still part of the mystery that we have to figure out.
Alternatively they could be another body spirochete (oral or gut) that explodes because of immunosuppression of LD>
Here is a BEAUTIFUL spiro in a LD patient blood, the same type we see in our blood, & it is caught undergoing a perfect cyst. This video is so precious & shows that this thing is a spirochete!
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
posted
BOOM!!!!
Dr. Alan MacDonald, THE GOD OF BORRELIA, strikes again & this time showing that Borrelia can be seen in the blood of someone who is long-term ill with Lyme Disease & where serology testing may be negative or inconclusive. Please, please, please donate if you have not already (I have )
The Lyme Disease Network is a non-profit organization funded by individual donations. If you would like to support the Network and the LymeNet system of Web services, please send your donations to:
The
Lyme Disease Network of New Jersey 907 Pebble Creek Court,
Pennington,
NJ08534USA http://www.lymenet.org/









 UBBFriend: Email this page to someone!
UBBFriend: Email this page to someone!








![[Smile]](smile.gif) )
)



 Printer-friendly view of this topic
Printer-friendly view of this topic