posted
That's actually pretty good. I am curious how it looks in 4k? Also, I would have to see the setup, as well as actually try it out first, if it is something he makes himself.
I wonder if it is just a camera type attachment that he makes? And not a full microscope system?
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
posted
I PM'd you his emails w/description.
Posts: 2094 | From NY | Registered: Oct 2011
| IP: Logged |
posted
I have zeroed in on a few prospects for microscopes. You can find quite a few serviceable, research grade microscopes from the 80s and 90s, still in use by labs, that are relatively affordable compared to the newest models.
I am seeking out those options, as they will provide the highest quality, highest resolution imaging.
We'll see how they pan out.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
Ha, I thought about posting the link to that one, too. Yes, someone will get a sweet machine. I am watching just to see how high (or low) it goes.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
posted
Thanks for the help in looking for scopes, guys. Input is always good.
I have put the money down for a new one.
I will unveil it when it is appropriate. Got's all kinds of goodies. I bought it used, but everything appears to be in new condition.
High quality lenses. Phase Contrast/Darkfield, DIC, Epi-Fluourescence, and standard Brightfield.
I am actually excited to play around with the DIC. Especially on a high quality. If you don't know what that is, just look it up. Very similar to standard Phase Contrast.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
quote:Originally posted by thatdudefromkansas: Thanks for the help in looking for scopes, guys. Input is always good.
I have put the money down for a new one.
I will unveil it when it is appropriate. Got's all kinds of goodies. I bought it used, but everything appears to be in new condition.
High quality lenses. Phase Contrast/Darkfield, DIC, Epi-Fluourescence, and standard Brightfield.
I am actually excited to play around with the DIC. Especially on a high quality. If you don't know what that is, just look it up. Very similar to standard Phase Contrast.
AWESOME!! You're making me drool. Would love to see a pic of it sometime. Can't wait to see some blood with it.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
posted
I'll post a video of the setup and get some BSK samples under it once it's all set up.
Start looking into getting some fluorescent stains and working through that process. Figuring out which, antibody-wise, to start out with.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
Interesting. Also note, Darkfield is preferred method for viewing the nematodes, no fixation or staining required.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
posted
Good stuff, thanks!
Interesting how there is a lot more buzz about Borrelia in the blood nowadays. Sounds like everyone's concerted efforts for recognition has started to pay off.
Posts: 2094 | From NY | Registered: Oct 2011
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
E-E-E-E-e-e-e-W-W-W-W-w-w-w-w !!!! THAT, is unmistakable! I'm glad I've never seen anything like that in my blood!!!
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
posted
Just took possession of an AO10... excited to re-read this thread and figure out how to get going.
Posts: 71 | From Canada | Registered: May 2016
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
quote:Originally posted by mustardseed2: Just took possession of an AO10... excited to re-read this thread and figure out how to get going.
Way to go, mustardseed2! Looking forward to hearing/seeing what you discover. Don't be afraid to ask questions or post any pics/videos.
Is your 10 equipped with either darkfield or phase contrast?
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
I might try a makeshift dark stop at some point for 40x, but I'm more interested in doing staining to check for co-infections.
Looking into how to do Giemsa now.
My first look at my blood cells, I didn't notice anything funny looking, except a couple of them had a large, black, bumpy, V-shaped inclusion. Not sure what those were.
Posts: 71 | From Canada | Registered: May 2016
| IP: Logged |
posted
So I saw my first potential spirochete tonight.
I haven't read this entire thread, so I'll go back and see if it matched what other people have seen.
It had bulbous tips, and sometimes looked like the string of pearls mentioned earlier. It was oscillating around quite quickly.
Are there any other organisms in the blood that could potentially look like this?
I also saw a couple that were shorter, with a bulb on each end and a short connection in between.
Posts: 71 | From Canada | Registered: May 2016
| IP: Logged |
bluelyme
Frequent Contributor (1K+ posts)
Member # 47170
posted
Congrats it is scary cool huh?..cant wait to get my own scope
-------------------- Blue Posts: 1539 | From southwest | Registered: Dec 2015
| IP: Logged |
I did several smears on the first day, and didn't find anything.
On Day 2 I re-checked the smears from Day 1, and still nothing. Then I made new smears, and still nothing.
Then before I went to bed, I did one more smear (this is 8 hours after my previous smear), and all of a sudden I could see a couple of them.
I'm going to draw more blood before bed tonight to see if there's a pattern or if it was coincidence.
edit: I also bought that camera stand from ebay for $20. It's coming from Chine though, so maybe by September I'll be able to post pictures haha.
Posts: 71 | From Canada | Registered: May 2016
| IP: Logged |
posted
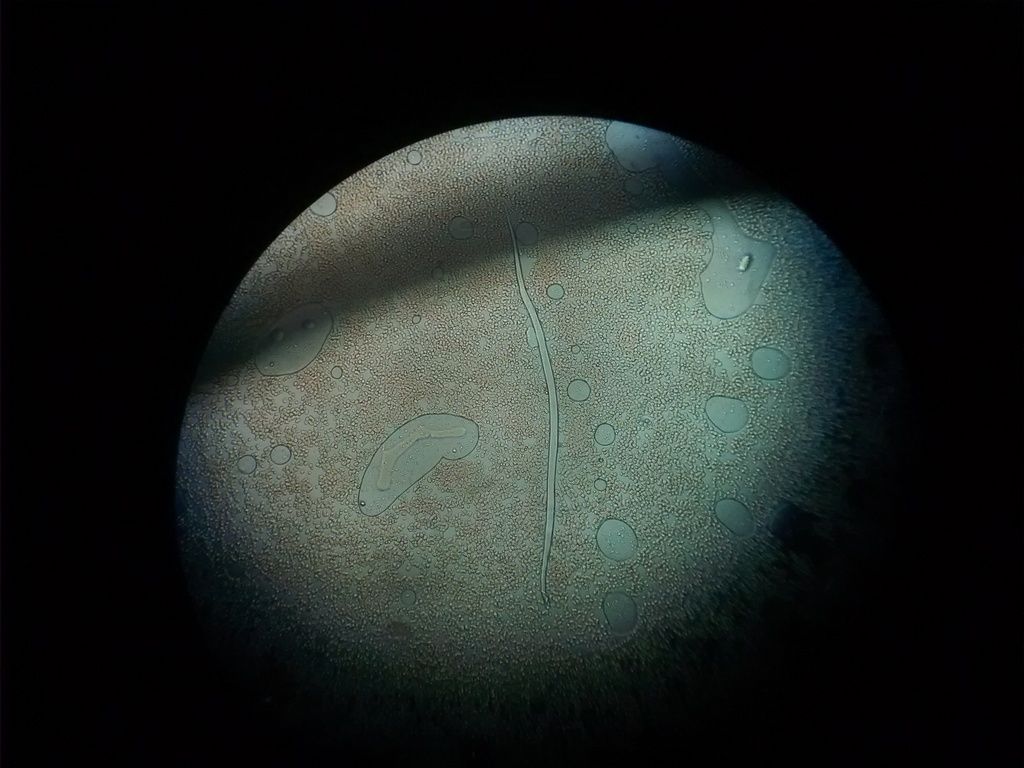
Check out this worm I found. Took the picture with my cell phone straight through the eyepiece.
10x objective 10x eyepiece
Posts: 71 | From Canada | Registered: May 2016
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
Interesting report! Sounds just like Bb....clinically & morphologically it is! It's interesting that they say most l-forms are not pathogenic except in rare cases! But, these sure caused symptoms!
Revista Brasileira de Reumatologia Print version ISSN 0482-5004 On-line version ISSN 1809-4570 Rev. Bras. Reumatol. vol.49 no.5 São Paulo Sept./Oct. 2009
IAssociate Rheumatology Professor of the Medical School of Universidade de São Paulo IIProfessor of Veterinary Medicine and Animal Health at the Faculdade de Medicina Veterinária e Zootecnia da Universidade de São Paulo IIIRetired Infectious Diseases Professor of Universidade Federal de São Paulo IVAssisting Physician of the Hospital das Clínicas of the Medical School of Universidade de São Paulo VRheumatology PhD student at the Medical School of Universidade de São Paulo VIBiologist of the Rheumatologic Investigation Laboratory of the Hospital das Clínicas of the Medical School of Universidade de São Paulo
Correspondence to
-----------------------------------------------
ABSTRACT
We report the unusual finding of mobile spirochetal microorganisms with different morphologies and sizes, on dark-field microscopy of the blood of animals from the Vivarium of the Medical School of USP. The bacteria did not grow in common culture media, shows faint staining to Giemsa and silver-derived stains, and serologies and molecular tests were negative for Borrelia and Leptospira.
Electron microscopy revealed the presence of microorganisms with Mycoplasma-like morphology and, due to its mobility, it was suggested that they represented Mollicutes of the genus Spiroplasma. Microorganisms with the same morphology were also observed in 15 out of 26 employees (57.6%) of the Vivarium of FMUSP; however, clinical and laboratorial exams indicated that those individuals were healthy.
Additional studies undertaken at the Rheumatology Department of FMUSP demonstrated the presence of the same structures identified at the Vivarium in approximately 94% of the patients with Baggio-Yoshinary syndrome (BYS) and 20% of healthy individuals. Electron microscopy of the blood of BYS patients showed bacteria that shared similarities with Mycoplasma, Chlamydia, and Bacteroides. Since serologies and molecular tests were negative for those contaminants, and based on publications in the medical literature, it was suggested that those latent infectious agents were L-form bacteria, defined as cell wall deficient bacteria, assuming, therefore, Mycoplasma morphology and they are, for the most part, harmless to the host.
We concluded that spirochetal microorganisms visualized in animals and employees of the Vivarium were non-pathogenic L-form bacteria from contaminants in the environment, regular infections, or endogenous microorganism from the normal saprophytic flora. On the other hand, spirochetal organisms identified in BYS, by preserving the capacity to invade cells in vitro, are potentially pathogenic and related to the etiology of BYS. We consider BYS as a novel Brazilian zoonosis caused by spirochetes adapted to their latent form, possibly due to bacterial mutations in response to ecologic and geographic conditions unique to Brazil.
On an administrative ruling published on 04/06/2002, the dean of USP, Professor Adolfo José Melfi, appointed Professors Natalino Hajime Yoshinari (Medical School of the Universidade de São Paulo - FMUSP), Silvio de Arruda Vasconcelos (Veterinary and Zootomy School of USP-FMZUSP), and Arary da Cruz Tiriba (Universidade Federal de São Paulo - UNIFESP) for a Commission created to investigate unusual bacteriological problems linked to Vivariums.
The problem in the Vivarium of FMUSP began in the beginning of 2001 when Dr. Ismar Cestari detected in vitro the presence of spirochete-like microorganisms in culture of spleen cells of an animal from the Vivarium of the Medical School of USP (FMUSP).
To understand the extension of the problem, the Commission examined the blood of the animals on dark-field microscopy and, indeed, confirmed the presence of spirochete-like microorganisms in 15 out of 15 mice blood samples (BALB/c, A/SNELL1, SWISS, and C57BI/6), in two out of 5 rat blood samples (WISTAR), five out of five rabbit blood samples, and in none of the guinea pig blood samples.
Blood samples were examined again on the second semester of 2002 and 28 out of 40 (70%) blood samples of different species of mice and rats were positive. The same procedure was used in animals from the Veterinary and Zootomy School of USP (FMVZUP, from the Portuguese) and dark-field microscopy showed "spirochetal structures" in only two out of eight mice blood samples and in none of the hamsters, indicating a problem of Vivariums, although this finding was more common at FMUSP.
Clinically, animals from the USP Vivarium were apparently healthy. The veterinary Sueli Blanes Dani et al.1 undertook preliminary biochemical analysis of serum pools of four female mice and five of WISTAR rats, showing increased levels of BUN, alkaline phosphatase, aspartate aminotransferase (AST), and alanine aminotransferase (ALT), suggesting the presence of some infectious or toxic factor responsible for the development of liver function-related biochemical disruption.
In the same study, electron microscopy and immunohystochemical tests of the lungs, liver, spleen, heart, and kidneys of the animals, and they identified Mycoplasma pulmonis in almost 100% of the animals in conventional vivariums, and in 18% of those that maintained adequate sanitary barriers. They stated that studies in the literature reported liver diseases caused by Mycoplasma in sheep, doves, and goats, but they did not find reports on rats. To confirm those findings, we repeated the electron microscopy of the blood samples of rodents with spirochetal organisms (Figure 1).
Since optical microscopy revealed the presence of mobile microorganisms of different sizes, ranging from miniscule dots to elongated structures reaching up to 15-20 µm, in the blood sample of the animals, the Commission initially thought they could be spirochetes. Serology for Leptospira and Borrelia, hemocultures in aerobic and anaerobic media and BSK, as well as molecular testing (PCR) for Leptospira and Borrelia, performed at FMUSP, FMVZUSP, and Biological Institute were persistently negative.
The uncommon size of the structures identified in the peripheral blood of the animals called the attention of the members of the Commission because they were large and apparently incompatible with Mycoplasma or Chlamydia. It was also interesting that it was difficult to cultivate those structures in common culture media and they were difficult to identify using stains like Giemsa, silver products, and vital stains, such as acridine orange. Those findings, associated with the absence of information in the medical literature, led many researchers to interpret those spirochetal structures as simple artifacts.
The major concerns were related to the anthropozoonotic aspects of this uncommon finding. Possible risks of this latent infectious process for employees who handled the animals, characterizing a work-related disease, as well as the interference of those contaminants on experimental studies, were hypothesized. It was interesting that animals underwent frequent bacteriological testing, but pathogenic microorganisms were never isolated. It is important to emphasize that the animals in the USP Vivarium were not isolated, nor were they "germ-free", besides being raised and kept in the Vivarium for approximately 20 years, except the dogs that are brought from outside the FMUSP complex.
The present study reports the problems and actions adopted by the Commission to answer the questions formulated by the Dean of USP regarding the risks to the employees and scientific investigations. The other objective was to discover the etiology and source of infection of the animals.
Due to the relevance of the subject, a complementary discussion resulting from the investigation of the Brazilian Lyme-like disease (Baggio-Yoshinari syndrome - BYS), which brought new understanding on the incidence of spirochetal organisms in laboratory animals and humans, was added. It was demonstrated that those structures are seen almost always in mammals, including humans (Figure 2A), and that they grow briefly in SP4 medium (Figure 2B).
When analyzed under electron microscopy, those structures are similar to Mycoplasma, which, in reality, represent microorganisms that lost the cellular wall (cell wall deficient bacteria or L-form) and are, for the most part, "harmless" to living beings. However, for unknown reasons, maybe due to ecologic and climatic factors inherent to the country, strong evidence indicate that the etiological factor of BYS is an atypical latent spirochete with characteristics suggestive of Mycoplasma, Chlamydia, and Bacteroides (Figures 3A, B, and C). However, since the structures isolated in BYS cases are capable of invading endothelial cells (Figure 4), it is believed that they are potentially pathogenic, justifying the clinical and laboratorial particularities of this emerging Brazilian zoonosis.
The objective of this study was to demonstrate that the description of "harmless" L-form microorganisms in living beings is common. But, in some situations, as in the Baggio-Yoshinari syndrome, cell wall deficient spirochete, possibly bacteria of the genus Borrelia, would preserve their pathogenic properties, causing an extremely morbid disease distinct from Lyme disease seen in the northern hemisphere.
PATIENTS AND METHODS
All employees of the FMUSP Vivarium, evaluated according to the study protocol determined by the Commission instituted by the Dean of USP, were included in this study to evaluate the health of the employees who handled the animals or worked at the Vivarium.
This protocol included a clinical investigation with complete history and physical exam. As for complementary exams, the following were evaluated: 1; Blood: CBC (automated test, microscopy, and Panotic stain); 2. Biochemical: BUN (kinetic assay), creatinine (colorimetric kinetic assay), glucose (colorimetric enzymatic assay), total cholesterol (colorimetric enzymatic assay), triglycerides (colorimetric enzymatic assay), uric acid (colorimetric enzymatic assay), sodium (ion-selective electrode assay), potassium (ion-selective electrode assay), calcium (colorimetric assay), serum iron (colorimetric assay), ALT (kinetic assay), AST (kinetic assay), gamma-glutamyl transferase (GGT - kinetic test), and creatine phosphokinase (CPK - kinetic test); 3. Urine analysis: urine type I; 4. Bacteriologic: hemoculture, coproculture (stool culture), and stool parasitologic (Leishman stain); 5. Immunologic and inflammatory: C-reactive protein (nephelometric assay), erythrocyte sedimentation rate (Westergren assay), C3 and C4 complement (nephelometric assay), protein electrophoresis, protein immunoelectrophoresis, rheumatoid factor (agglutination assay), antinuclear factor in Hep-2 cells (immunofluorescence assay), and anti-streptolysin O (nephelometric assay); 6. Serologies for infectious diseases: Lyme disease, at the Medical Investigation Laboratory (LIM-17, from the Portuguese) of HCFMUSP (immunoenzymatic assay - ELISA), leptospirosis, at the FMVZUSP (microscopic seroagglutination assay), and the remaining assays for syphilis (immunoenzymatic assay - ELISA), toxoplasmosis (microparticle immunoenzymatic assay - MEIA), hepatitis A and B (microparticle immunoenzymatic assay - MEIA), hepatitis C (chemiluminescence assay), and cytomegalovirus (immunoenzymatic assay - ELISA) at the Central Laboratory of HCFMUSP; 6. Imaging exams: chest X-ray and abdominal ultrasound (US) scan; and 7. Specialized medical evaluation when necessary.
This study was approved by the Ethics Commission for the Analysis of Experimental Studies - CAAPPesq (from the Portuguese) of HCFMUSP (342/09).
RESULTS
Thirty-seven employees of the FMUSP Vivarium, five of which were administrative employees, were evaluated at the Internal Medicine Outpatient Clinic of the Hospital das Clínicas of FMUSP. Since this was a conventional Vivarium, without isolation areas, the employees were not discriminated according to their position. Twenty-five were males and 12 females; their age ranged from 21 to 54 years (36.6 ± 9.87).
HISTORY
Twelve out of 27 (32.4%) employees complained of some allergic manifestation, such as asthma, rhinitis, or skin eruption. The frequency of "social drinking" was 62.5%, i.e., 15 out of 24 individuals who answered this question.
Out of 37 employees interviewed, ten complained of frequent fatigue and asthenia (27%), while three (8.1%) referred recurrent episodes of fever or chills.
As for the locomotor system, nine (24.5%) complained of constant back pain, eight (21.6%) had arthralgias, two had talalgia, and one had arthritis and myalgia. Sixteen employees (43.2%) did not have osteoarticular symptoms.
Regarding neurological manifestations, 12 (32.4%) employees had headaches regularly, nine (24.3%) reported being forgetful, seven (18.9%) had sleep problems, five (13.5%) were nervous or irritable, three (8.1%) had lack of concentration, three (8.1%) experienced episodes of dizziness, and one had facial paralysis. Nine employees (24.3%) denied having any neurological symptoms.
As for cardiovascular symptoms, five employees (13.5%) experienced frequent episodes of palpitations and three (8.1%) had atypical chest pain.
Review of the other systems showed that 12 (32.4%) complained of increased in the daily number of evacuations (more than two), six (16.2%) had sore throat frequently, and four reported constant episodes of coughing or upper airways infection. Five (13.5%) employees did not have any clinical complaints.
PHYSICAL EXAM
The physical exam did not show significant changes; cutaneous manifestations were observed in five patients (pustules, erythema macular, hyperhidrosis, pityriasis versicolor, and psoriasis). One employee had hepatomegaly and clubbing of the fingers, lung auscultation was compatible with bronchospasm in one employee, another had arthritis compatible with gout, and one had Heberden and Bouchard nodes (arthrosis of the hands).
LABORATORIAL TESTS
Complete blood count was normal, except in two cases in which it showed mild leukocytosis, three had leucopenia, and five had mild anemia. Changes in platelet count were not observed.
Table 1 shows the main results of blood biochemistry, and the number of employees with increased levels of liver and muscle enzymes is striking.
INFLAMMATORY ACTIVITY AND IMMUNOLOGIC TESTS
Table 1 shows the changes in inflammatory activity and immunologic tests of the employees of the FMUSP Vivarium. Note that 26% of the employees presented positive C-reactive protein and 36% had increased IgE.
SEROLOGIES FOR INFECTIOUS DISEASES
Table 2 shows the results of the serologies for the Brazilian Lyme-like disease, leptospirosis, syphilis, toxoplasmosis, hepatitis A, B, and C, and cytomegalovirus. The frequency of sera positive for Borrelia burgdorferi was similar to that observed in the normal control population. One patient tested positive for syphilis and two for toxoplasmosis, being referred to the Infectious Disease Department.
BACTERIOLOGY AND STOOL PARASITOLOGY
Table 2 describes the bacteriological and stool parasitologic tests, visualization of spirochetal structures on dark-field microscopy, and PCR for leptospirosis of the employees of FMUSP Vivarium. Blood cultures and coprocultures were negative; spirochetal structures were observed in 57.6% of the cases (Figure 2A), and the presence of Blastocystis hominis was demonstrated in 12% of the employees analyzed. Stool leukocytes were present in 36% of the cases.
IMAGING
Chest X-ray was normal in all employees who underwent this exam. Total abdominal US showed some changes in 10 out of 18 cases (55.5%), and the abnormalities observed included: hepatic steatosis in five cases, liver enlargement in four cases, peripancreatic lymph nodes in one case, hepatic calcifications in one case, dilated common hepatic duct in one, and hepatic nodules in one employee.
LIVER EVALUATION
Employees with abnormal abdominal US were referred to the gastroenterologist, but significant changes, deserving complementary investigation, were not observed.
DISCUSSION
A large number of professionals of different Research Institutions was mobilized to study the clinical condition of the employees of the USP Vivarium due to the uncommon finding of latent microorganisms in the animals of that institution, which might indicate an emerging zoonosis and a new work-related disease. Since references on microorganisms, with the characteristics described here, in the blood of animals and humans, were not found in the medical literature, it was very difficult to explain where they came from and what would be the pathogenic role of those microorganism in the host.
An explanation was urgently needed, not only to reassure the employees regarding the risks to their health, but also to inform the scientists of the institution who used animals from the Vivarium of any interferences of this infection on animal research.
The poor sanitary conditions of the Vivarium suggested that environmental factors could be influencing the development of those spirochetal structures, since the frequency of contaminants varied among the institutions investigated. It was surprising that the same structures present in animals were identified in 15 out of 26 employees (57.6%), indicating possible work-related transmission of those microorganisms.
The Commission also observed that the employees of the Vivarium had poor hygiene, since they ate and slept in the work place, sometimes manipulated animals without gloves, they did not wear boots when they were in direct contact with animal waste, and promiscuity among the different animal species was also observed. Therefore, educating the employees on proper hygiene and establishing strict rules regarding animal care were the first steps taken.
The medical exam of the employees demonstrated that they were in good clinical condition; however, the high frequency of allergic phenomena and diarrhea was striking. As for the laboratorial work up, some individuals had abnormal inflammatory activity assays, elevated liver and muscle enzymes, high levels of IgA and IgE, and leukocytes in the stools. Initially, we thought we were seeing a higher incidence of liver, intestinal, and allergic complications. However, this impression was not confirmed due to the lack of a control group, with the same demographic characteristics and habits, but not working at the Vivarium.
Some aspects stood out, such as the high incidence of social drinking (62.5%), continuous exposure of the employees to animal waste, rations, and different biological products, besides the poor hygiene of those individuals. We thought those factors partly explained the clinical complaints and laboratorial changes seen, and that preventive measures would contribute to reduce the incidence of animal and human infection, in addition to the "eventual normalization" of the abnormal tests. We were reassured when employees whose abdominal US and laboratorial tests indicated hepatic changes were evaluated by the Gastroenterology Department of HCFMUSP and were considered normal, without the need of further procedures.
The next step of the study was to try to elucidate the etiology of the latent infection demonstrated by the finding of spirochetal structures in animals and employees of the Vivarium (Figure 2A). They were of different sizes and morphologies, mobile, nonculturable, did not stain by the Giemsa method and, although they resembled spirochetes, laboratorial tests were persistently negative for Leptospira and Borrelia. Serologies for the Brazilian Lyme-like disease, leptospirosis, and syphilis were negative, as well as molecular biology tests for Leptospira spp. and Borrelia spp. (data not presented).
As mentioned before, Damy SB et al.1 identified Mycoplasma pulmonis in 100% of laboratory animals raised conventionally, and they reported that those microorganisms could cause hepatic damage, justifying the enzymatic changes seen in the animals of the FMUSP Vivarium.
Mycoplasmata are considered the smaller self-replicating organisms, require cholesterol for their survival, and do not have cellular wall. Similar to Chlamydiae, they are intracellular organisms that infect several cells, such as endothelial and epithelial cells, and macrophage, besides representing important co-factors of the increased virulence of infections caused by other microorganisms2. Higuchi et al.3,4 reported that those microorganisms influence the development of unstable atheroma plaques. They were able to visualize, on electron microscopy, elliptical and cylindrical forms of Mycoplasmata of different sizes distributed in the extracellular matrix of affected human tissues.
However, we did not find any references in the medical literature to the possible role of Mycoplasma spp. and Chlamydia spp. as zoonotic agents. It was also intriguing that those microorganisms were minute and non-mobile, contradicting the findings of dark-field microscopy, which revealed mobile structures measuring up to 15 µm in length. Thus, the hypothesis that the microorganisms identified in the blood of rodents from the FMUSP Vivarium (Figure 1) were Mycoplasmata was not confirmed. According to the personnel of Professor J. Timenetsky of ICBUSP, a specialist in Mycoplasmata, the majority of rodents is infected by these bacteria and, therefore, the findings on electron microscopy could be incidental, not related to our findings.
But we investigated the possibility of finding mobile bacteria with greater dimensions and Mycoplasma morphology. It is known that the Mollicutes group of bacteria is composed by Mycoplasma, Spiroplasma, and Acholeplasma, cell wall deficient microorganisms surrounded by a cholesterol-rich cellular membrane. According to Shlomo T & Rami G5, microorganisms of the genus Spiroplasma show circular and elliptical movement due to the presence of a cytoskeleton that works as a propeller, and they have chemotactic properties. They can reach up to 10 µm in length, are sensitive to erythromycin and tetracyclines, and some species are pathogenic for rats, mice, hamsters, and rabbits. They can also be identified in plants, bees, ticks, wasps, and mosquitoes6. It is curious that several Spiroplasma cells contain a virus (SpV)7, whose pathogenic meaning is unknown.
Since the Mollicutes hypothesis might not be completely satisfactory, the Commission considered other agents with similar morphology to that of spirochetes on dark-field microscopy. Among other possibilities, we thought of mobile spiral microorganisms, such as Helicobacter spp8., Serpuline spirochetes9, and Anaerobiospirillum10, whose common trait includes difficulty growing in usual media and their role on the pathogenesis of human and animal infirmities. Spirochetes of the genus Serpulina live in the digestive tract of animals, causing diarrhea11,12, and immunosuppressed patients may be equally infected by those difficult to diagnose spirochetes12. Additionally, it is known that several spirochetes are among the oral saprophytic flora of normal individuals13; however, we did not know whether those microorganisms would be able to invade the blood stream and express as spirochetal structures.
Despite different etiologic possibilities, none was satisfactory, except for the possibility that they might be Spiroplasmas, mobile microorganisms similar to Mycoplasma. The other microorganisms mentioned have extremely different morphology on electron microscopy, since they have cellular wall, some of them have flagella, and they are extremely small (except for the genus Serpulina/Brachyspira).
Based on the data collected and information available, we concluded that a latent infection, which has not been described yet, caused by bacteria morphologically similar to Mollicutes, i.e., cell wall deficient, was present in animals and employees of the Vivarium. Due to the electron microscopic morphology of the microorganisms, the possibility of infection by the Spiroplasma genus was suggested. The medical evaluation of the employees allowed the prediction that those latent bacteria have a low pathogenic potential, but extended follow up of those individuals is warranted. As for animal studies, the Commission suggested the continuation of the studies since animals from other vivariums were also contaminated and, apparently, they were all in good physical condition.
The commission also recommended the urgent improvement of hygiene conditions of the employees, modernization and reformulation of the Vivarium, and stricter sanitary conditions as useful preventive measures to reduce the severity and frequency of contaminations. Although animal studies were not formally contraindicated, the members of the Commission reminded investigators that specific studies that depend on the total lack of microorganisms could be influenced by this latent infection. However, due to the characteristics of this infection, i.e., silent, occult, difficult to control, besides being disseminated among different vivariums, the Commission raised the possibility that this infection could be present in axenic or germ-free animals.
COMPLEMENTARY DISCUSSION ABOUT NEW KNOWLEDGE ON THE BAGGIO-YOSHINARI SYNDROME
The manuscript above, with some modifications, represents the Report sent to the Dean of USP and presented to the researchers of FMUSP, who use regularly animals from the Vivarium, and its employees.
Discovering the etiology of the Brazilian Lyme-like disease (BLLD), or Baggio-Yoshinari syndrome14, has been a great challenge. There are no doubts that symptoms compatible with Lyme disease, including typical erythema migrans and the development of multiple systemic complications, are seen in Brazil15,16. Unlike LD, the etiological agent of BYS has never been identified by microbiological (cultures) and molecular (PCR) methods17.
Thus, in our opinion, this marked difference in the etiology of both tick-transmitted zoonoses would justify the large number of clinical and laboratorial particularities between the diseases seen in Brazil and the northern hemisphere. Clinically, the Brazilian zoonosis has a high incidence of relapses, which is rare in LD. As for laboratory exams, patients with BYS have low immunological reactivity to Borrelia burgdorferi sensu lato antigens and high frequency of autoimmune disorders, such as the development of autoantibodies against neuronal elements18.
We believe that, despite the differences, BYS is a zoonosis caused by spirochetes. We postulate that, due to the geographical, climatic, and ecological conditions seen in Brazil, such as the absence of the Ixodes ricinus tick, the main vector of LD in the northern hemisphere19, conditions for the development of exotic spirochetes, maybe mutants, capable of surviving in vertebrate and invertebrate hosts in the country, do exist. Currently, we know that Borrelia organisms are capable of modifying their genome and proteome during their life cycle, which involves infection of ticks and animals20,21,22,23,24,25.
To identify the etiological agent of BYS in the peripheral blood of affected patients on dark-field microscopy, we identified similar spirochetal structures in animals and employees of the Vivarium of FMUSP. Similarly, spirochetal organisms from patients with BYS did not grow in BSK medium or in any of several other culture media tested.
Initially, based on the conclusions of the report given to the Dean of USP, we believed those structures to be Mollicutes of the genus Spiroplasma. And reinforcing this hypothesis, we discovered that those latent bacteria were capable of growing and surviving for approximately 10 days in adequate medium for the development of Spiroplasma, known as SP4 (Figure 2B). On the other hand, seeding spirochete of the Borrelia burgdorferi sensu lato complex in SP4 medium caused their cellular degeneration to the point that they lost their typical helicoidal movement and became similar to those structures seen in BYS and in the animals of the Vivarium.
The presence of those latent microorganisms in the blood of normal individuals who were not employees of the Vivarium and who did not have a history of recent tick bite was a surprising finding. Upon investigating those structures in 52 patients with BYS and in 50 healthy individuals, we demonstrated the presence of those spirochetal structures in 49 of 52 (94.2%) samples of patients with BYS and in only 20% of healthy individuals (non-published data).
Analyzing the spirochetal structures seen in BYS on electron microscopy, Mantovani et al.26 visualized microorganisms whose morphology was suggestive of Mycoplasma, Chlamydia, and spirochetes. This discovery led the authors to assume that the etiology of BIS would be linked to this diversity of latent microorganisms, characterizing a new tick-transmitted clinical entity. Additionally, the discovery that those latent microorganisms isolated in patients with BYS were capable of infecting endothelial cells in vitro, indicating that they are potentially pathogenic, was also very relevant (unpublished data) (Figure 4).
When we performed serologies and molecular biology testing (PCR) for Mycoplasma spp. and Chlamydia spp. in patients with the BLLD and healthy subjects, we noticed that the behavior in both groups was similar, indicating that those spirochetal structures were not the microorganisms imagined previously (unpublished data). At that moment, the hypothesis that those latent bacteria belonged to genera Mycoplasma and Chlamydia lost strength. By analogy, the hypotheses that animals and employees of the Vivarium were contaminated by Mollicutes of the genus Spiroplasma was also under suspicion.
Searching for answers, we discovered, after a deep review of the medical literature, that all bacteria can assume Mycoplasma morphology when they lose components of the cellular wall, which might happen in adverse conditions27,28,29. Those morphologically altered bacteria, structurally similar to Mycoplasma, are known as L-form, spheroplasts or cell wall deficient bacteria. This phenotypic change is also observed in spirochetes of the genera Treponema and Borrelia30,31,32.
When spirochetes are cultivated under adverse conditions of pH, temperature, or in the presence of antibiotics, they undergo important morphological changes, giving rise to atypical structures of different sizes and shapes, ranging from miniscule dots and spores (known as blebs) to formations resembling elongated bacteria (spirochetal), dense corpuscles with a double membrane (similar to Chlamydia), and single-membrane cysts (suggestive of Mycoplasma) on electron microscopy33. Additionally, the presence of spirochetes with atypical morphology, such as those mentioned above, in the brain parenchyma of patients with neurological manifestations of syphilis and Lyme borreliosis, has been described34,335. Under favorable culture conditions, L-form spirochetes reassume the normal helicoidal morphology36.
The medical literature considers most L-form bacteria nonpathogenic, with rare exceptions27. The aggregated knowledge of LIM-17 HCFMUSP led us to postulate that the presence of L-form bacteria in animals and humans would be relatively common. We considered that regular and transitory infections of the respiratory, digestive, and urinary tract would be the usual source of contamination. Places with improper sanitary conditions, such as those found in the FMUSP vivarium, would certainly present a high environmental bacterial proliferation, as well as contamination of humans and animals, leading to a high incidence of spirochetal structures (L-form bacteria) in the peripheral blood. The normal saprophytic flora would be another suggested source of spirochetal structures.
In most cases, L-form microorganisms are not pathogenic, as we mentioned on our report to the Dean of USP. However, in our opinion, the behavior of spirochetal structures found in BYS is different than normal since, by preserving the ability to invade endothelial cells, they reveal a high pathogenic potential. Since spirochetes in their helicoidal form were never cultivated and isolated in Brazil, we assumed that the etiology of BYS was linked to L-form spirochetes. We believe that the etiological agent of BYS adapted permanently to its atypical morphology due to the irreversible loss of genetic and cell wall lipoprotein contents (Osp) in order to survive in adverse conditions, such as the absence of Iodes ricinus ticks in Brazil. Recent publications demonstrated that the genetic diversity of different species of Borrelia burgdorferi sensu lato complex spirochetes is subjected to regional and continental influences37,38,39.
Finally, by accepting that BYS is caused by atypical spirochetes, we are able to justify all clinical and laboratorial particularities of this Brazilian zoonosis. This theory explains the clinical relapses and evolution of BYS into the so called idiopathic chronic disorders; treatment difficulties, especially in chronic diseases; the interference of microorganisms on the immune system, leading to the development of immune-allergic reactions; why those bacteria are difficult to grow in different media and stain poorly by common staining methods; why those microorganisms cause low immunologic reactivity to Borrelia burgdorferi; and why molecular tests, such as PCR, are persistently negative, possibly due to the partial loss of plasmids.
The theory that, in Brazil, BYS is caused by a mutant spirochete, genetically modified, and devoid of most of the cellular wall (Osp) and periplasmic flagella, is supported by the medical literature, since a mutant form of Borrelia burgdorferi and deficient on Osp, A, B, C, and D, has been described40. Those surface proteins are important to distinguish the different species of spirochetes of the Borrelia burgdorferi sensu lato complex and they participate on the pathogenicity and triggering of immunologic host reaction to the microorganism. Additionally, the mobility and helicoidal form of Borrelia are dependent on the 7-11 periplasmic flagella41,42, and when mutation of the flab gene (main flagellin gene) is present, the spirochete assumes a bacteroid morphology43, resembling the electron microscopic shape visualized in Brazil. Thus, spirochetes that have lost their flagella and wall lipoproteins would assume a spirochetal aspect, on dark-field microscopy, and an aspect of Mycoplasma and Chlamydia, on electron microscopy.
Today, after 20 years of investigations, we dare to define BLLD, or BYS, as an original Brazilian disorder caused be latent bacteria with atypical L-form morphology, transmitted by ticks that do not belong to the Ixodes ricinus complex, that produces clinical manifestations similar to those observed in LD, except for the high incidence of relapses, and a tendency for chronicity and immune-allergic reactions.
ACKNOWLEDGMENTS
Professor Flair Carrilho, MD - Professor of the Gastroenterology Department of FMUSP
Professor Milton Arruda Martins, MD - Professor of Internal Medicine of FMUSP
Dr. José Antonio Atta - Collaborating Professor of FMUSP
Professor Maria de Lourdes Higuchi, MD - Associate Professor of INCOR FMUSP
Eliana Scarcelli Pinheiro - Scientific Researcher of the Biological Institute
Margareth Elide Genovez - Scientific Researcher of the Biological Institute
Professor Paulo Yasuda, MD - Retired Professor of ICB USP
Professor Silvia Barreto C. Ortiz - Responsible for the Vivarium of FMUSP
Robson José da Cruz - Biologist of the Vivarium of FMUSP
Sueli Blanes Damy - Veterinarian of the Vivarium of FMUSP
Dr. Cristiano Correa de Azevedo Marques - General Director of the Adolfo Lutz Institute
Dr. Vera Simonsen - Head Bacteriologist of the Adolfo Lutz Institute
REFERÊNCIAS
1. Damy SB, de Lourdes Higuchi M, Timenetsky J, Sambiase NV, Reis MM, Ortiz SC. Co-infection of Laboratory Rats with Mycoplasma pulmonis and Chlamydia pneumoniae. Contemporary Topics. 2003; 42:52-6. [ Links ]
2. Razin S, Yogev D & Naot Y. Molecular biology and pathogenicity of mycoplasms. Microbiology and Molecular Biology Reviews. 1998; 62:1094-156. [ Links ]
3. Higuchi M, Castelli JB, Aiello VD, et al. Great amount of C. pneumoniae in ruptured plaque vessel segments at autopsy. A comparative study of stable plaques. Arq bras Cardiol. 2000; 74: 149-11. [ Links ]
4. Higuchi ML, Sambiase N, Palomino S, et al. Detection of Mycoplasma pneumoniae and Chlamydia pneumoniae in ruptured atherosclerotic plaques. Braz J med biol Res. 2000; 33: 1023-26. [ Links ]
5. Shlomo T & Rami G. A bacterial linear motor: cellular and molecular organization of contractile cytoskeleton of the helical bacterium Spiroplasma melliferum BC3. 2001; 41:827-48. [ Links ]
6. Regassa LB, Gasparich GE. Spiroplasmas: evolutionary relationships and biodiversity. Front Biosci.2006; 11:2983-3002. [ Links ]
7. Renaudin J, Bové JM. SpV1 and SpV4, Spiroplasma viruses with circular, single-strained DNA genomes, and their contributions to the molecular biology of Spiroplasmas. Adv Virus Res. 1994; 44:429-63. [ Links ]
8. Fox JG. The non H pylory helicobacters: their expanding role in gastrointestinal and systemic diseases. Gut. 2002; 273-83. [ Links ]
9. Scarcelli E, Bersano JG, Genovez ME, Mandorino I. Presença de Campylobacter hyointestinalis e Serpulina hyodysenteriae em um suíno oriundo de um surto de gastroenterite. Arq Inst Biol. 1995; 62:97-100. [ Links ]
11. Mikosza AS, Hampson DJ. Human intestinal spirochetosis: Brachyspira aalborgi and/or Brachyspira pilosicoli ? Anim Health Res Rev. 2001; 2:101-10. [ Links ]
12. Smith JL. Colonic spirochetosis in animal and humans. J Food Prot. 2005; 68:1525-34. [ Links ]
13. Schuster GS. Oral flora and pathogenic organisms. Infect Dis North America. 1999; 13:757-74. [ Links ]
14. Gauditano G, Bonoldi VLN, Costa IP et al. Síndrome de Lymesímile ou complexo infecto-reacional do carrapato ou Síndrome Baggio-Yoshinari. Rev Paulista Reumatol. 2005; 4:16-7. [ Links ]
15. Yoshinari NH, Barros PJL, Bonoldi VLN. Perfil da borreliose de Lyme no Brasil. Rev Hosp Clin Fac Med S Paulo 1997; 52:111-7. [ Links ]
16. Costa IP, Bonoldi VLN, Yoshinari NH. Perfil clínico e laboratorial da Doença de Lyme-símile no Estado de Mato Grosso do Sul: análise de 16 pacientes. Rev Bras Reumatol. 2001; 41:142-50. [ Links ]
17. Costa IP, Bonoldi VLN, Yoshinari NH. Search for Borrelia sp in ticks from potential reservoir in an urban forest in the State of Mato Grosso do Sul, Brazil: a short report. Mem Inst Oswaldo Cruz. 2002; 97:631-5. [ Links ]
18. Gauditano G, Bonoldi VLN, Hiratsuka RC, Kiss MH, Yoshinari NH. Aspectos imunológicos comuns entre a Doença de Lyme e a Febre Reumática. Rev Bras Reumatol. 2000; 40:1-7. [ Links ]
19. Lane RS, Piesman J, Burgdorfer W. Lyme borreliosis: relation of its causative agent to its vectors and hosts in North America and Europe. Annu Rev Entomol. 1991; 36:587-609. [ Links ]
20. de Silva AM, Fikrig E. Arthropod and host-specific gene expression by Borrelia burgdorferi. J Clin Invest. 1997; 99:377-9. [ Links ]
21. Schwan TG, Piesman J. Temporal changes in outer surface proteins A and C of the Lyme disease-associated spirochete, Borrelia burgdorferi, during the chain of infection in ticks and mice. J Clin Microbiol. 2000; 38:382-8. [ Links ]
22. Hovius JW, van Dam AP, Fikrig E. Tick-host-pathogen interactions in Lyme borreliosis. Trends Parasitol. 2007; 23:434-8. [ Links ]
23. Hyde JA, Trzeciakowski JP, Share JT. Borrelia burgdorferi alters its gene expression and antigen profile in response to CO2 levels. J Bacteriol. 2007; 180:437-5. [ Links ]
24. Yang X, Goldberg MS, Popova TG et al. Interdependence of environmental factors influencing reciprocal patterns of gene expression in virulent Borrelia burgdorferi. Mol Microbiol. 2000; 37:1470-9. [ Links ]
26. Mantovani E, Costa IP, Gauditano G, Bonoldi VLN, Higuchi ML, Yoshinari NH. Description of Lyme disease-like syndrome in Brazil. Is it a new tick borne disease or Lyme disease variation? Braz J Med Biol Res 2007; 40:443-56. [ Links ]
27. Dominique GJ, Wood HB. Bacterial persistence and expression of disease. Clin Microbiol Ver 1997; 10:320-44. [ Links ]
28. Alla EJ, Hoischen C, Gumper J. Bacterial L form. Adv Appl Microbiol 2009; 68:1-39. [ Links ]
29. Austrauskiene D, Bernotiene E. New insights into bacterial persistence in reactive arthritis. Clin Exp Rheumatol 2007; 25:470-9. [ Links ]
30. Mursic VP, Wanner G, Reinhardt S, Wilske B, Busch U, Marget W. Formation and cultivation of Borrelia burgdorferi spheroplast-L-form variants. Infection. 1996; 218-6. [ Links ]
31. Murgia R, Cinco M. Induction of cystic forms by different stress conditions in Borrelia burgdorferi. APMIS. 2004; 112:57-62. [ Links ]
32. Ovcinnikov NM, Delektorskij VV. Current concepts on the morphology and biology of Treponema pallidum based on electron microscopy. Br J Vener Dis. 1971; 47:315-28. [ Links ]
33. Kersten A, Poitschek C, Rauch S, Aberer E. Effects of penicillin, ceftriaxone, and doxycycline on morphology of Borrelia burgdorferi. Antimicrobial Agents & Chemotherapy. 1995; 39: 1127-33. [ Links ]
34. Miklossy J, Kasas S, Zurn AD, McCall S, Yu S, McGeer PL. Persisting atypical and cystic forms of Borrelia burgdorferi and local inflammation in Lyme neuroborreliosis. J Neuroinflammation. 2008; 5:40; published online doi: 10.1186/1742-2094-5-40 [ Links ] 35. Duray PH, Yin SR, Ito Y et al. Invasion of human tissue ex vivo by Borrelia burgdorferi. J Infect Dis 2005; 191:747-54. [ Links ]
36. Brorson O, Brorson S. A rapid method for generating cystic forms of Borrelia burgdorferi, and their reversal to mobile spirochetes. APMIS 1998; 106:1131-41. [ Links ]
37. Derdáková M, Lencáková D. Association of genetic variability within the Borrelia burgdorferi sensu lato with the ecology, epidemiology of Lyme borreliosis in Europe. Ann Agric Environ Med. 2005; 12:165-72. [ Links ]
38. Kurtenbach K, Hanincová K, Tsao JI, Margos G, Fish D, Ogden NH. Fundamental processes in the evolutionary ecology of Lyme borreliosis. Nature Reviews/Microbiology. 2006; 4:660-9. [ Links ]
39. Malawista SE, Montgomery RR, Wang XM, Fu LL, Giles SS. Geographic clustering of an outer surface protein A mutant of Borrelia burgdorferi. Possible implications of multiple variants for Lyme disease persistence. Rheumatology. 2000; 39:537-41. [ Links ]
40. Sadziene A, Denée T, Barbour AG. Borrelia burgdorferi mutant lacking Osp: Biological and Immunological characterization. Infection and Immunity. 1995; 63:1573-80. [ Links ]
41. Sal MS, Li C, Motalab MA, Shibata S, Aizawa S, Charon NW. Borrelia burgdorferi uniquely regulates its motility genes and has an intricate flagellar hook-basal body structure. J Bacteriol. 2008; 190:1912-21. [ Links ]
42. Motaleb MA, Corum L, Bono JL et al. Borrelia burgdorferi periplasmic flagella have both skeletal and motility functions. Proc Natl Acad Sci USA. 2000; 97:10899-904. [ Links ]
43. Motaleb MA, Sal MS, Niles WC. The decrease in FlaA observed in a flaB mutant of Borrelia burgdorferi occurs posttranscriptionally. J Bacteriol. 2004; 186:3703-11. [ Links ]
Correspondence to: Prof. Natalino Hajime Yoshinari Av. Dr. Arnaldo 455, sala 3184 Cerqueira Cesar, SP - CEP: 01246-903 E-mail: yoshinari@ lim17.fm.usp.br
Received on 6/23/2009. Approved on 8/12/2009.
Study undertaken at the Rheumatology Department of the Medical School of Universidade de São Paulo with a grant from the Research Support Foundation of São Paulo (FAPESP, from the Portuguese).
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
Sorry about the mix-up with my post. I had posted it earlier and forgot some images and tables. When I went back to add them, I could only access a small portion of my original post. So, I had to re-post it with the added items.
Does this describe the pathology, virulence, and clinical picture of Bb? Seems to me to be a CARBON COPY. You'll never find this much info about Bb in the medical journals, though. No way. The only person that published this much info about Bb is Lida Mattman in her Stealth Pathogens book. And, she goes into even more detail about Bb....
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
quote:Originally posted by mustardseed2: Check out this worm I found. Took the picture with my cell phone straight through the eyepiece.
10x objective 10x eyepiece
Mustardseed, I don't mean to diminish your enthusiasm, but what do the tips of that object look like under greater magnification? Could it possibly be a paper fiber or small hair? I've seen a few of those in my samples already.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
posted
I suppose you could be right. Here's pictures of either end. Let me know what you think
Posts: 71 | From Canada | Registered: May 2016
| IP: Logged |
bluelyme
Frequent Contributor (1K+ posts)
Member # 47170
posted
Ooohh ..lots of acanthocytes...looks kinda like a filiarial.. ideas on species? ..how sick are you mustard ? Are you on any anti helminith (ivermectin and the like? )
-------------------- Blue Posts: 1539 | From southwest | Registered: Dec 2015
| IP: Logged |
posted
Good post, TNT. Always interesting to read those reports.
Mustard, as you become more proficient, things become much clearer and readily understood.
Be WEARY of viewing things like that, and understand that often times paper fibers (like those from lens paper, etc), have a similar appearance.
Keep up the good work, and approach everything objectively. Not diminishing, but you become more readily able to differentiate debris/contaminants/etc from things that are viable/living. Keep this in mind.
Can't say for sure what it is. If/when you get camera stand, it would be interesting to view things things under video as well.
Maintain enthusiasm.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
posted
Also, Mustard. What microscope setup do you currently have?
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
bluelyme
Frequent Contributor (1K+ posts)
Member # 47170
posted
quote:Originally posted by mustardseed2: Just took possession of an AO10... excited to re-read this thread and figure out how to get going.
-------------------- Blue Posts: 1539 | From southwest | Registered: Dec 2015
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
Dude, do you have any footage from the new scope?
I am amazed that your new scope wasn't put up for sale for $30-40,000.00 (as the ad said it was worth)! Did you pay more, or less, than the sale price listed? You still got an unbelievable deal if you paid anywhere close to the selling price listed.
It's too bad I don't live in Kansas, because I'd be driving over to get a peak through those lenses if I did!
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
posted
Yup it's AO10, with a blue filter. It's too bad I can't tell if it's a fiber, or if it's something cooler like a worm.
I'm not terribly sick, just have chronic 24/7 headache, tinnitus, weakness in my legs, and what appears as pink eye.
Acanthocytes.... hmmm... I thought the blood cells just showed up spiked like that because I haven't had much practice at staining and was messing something up... anything more you can tell me about these???
Posts: 71 | From Canada | Registered: May 2016
| IP: Logged |
bluelyme
Frequent Contributor (1K+ posts)
Member # 47170
posted
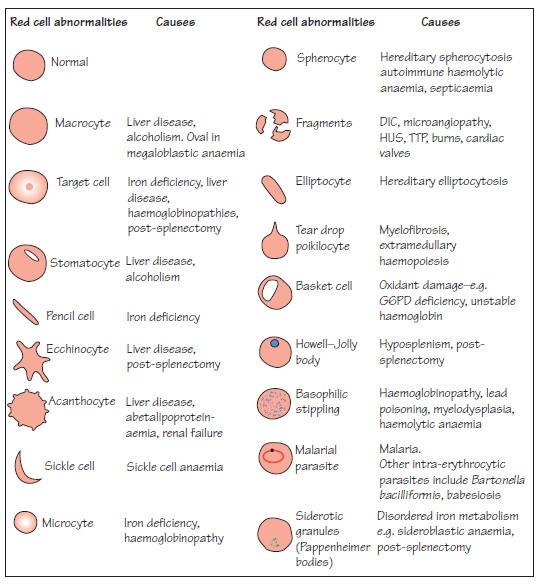
quote:Originally posted by WakeUp: One last red blood cell abnormality chart for your interest/review-- I find it interesting that the "malarial infected" cell is lumped in/similar to Bartonella and Babesia on this chart:
Oh probably cell damage i didnt know sample was altered
-------------------- Blue Posts: 1539 | From southwest | Registered: Dec 2015
| IP: Logged |
posted
Nope, I'll be testing it out at the end of the week/next week.
And I paid significantly less than that.
I won't be working with any stains for a bit, however.
Maybe next month some point.
Posts: 163 | From USA | Registered: Oct 2015
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
quote:Originally posted by thatdudefromkansas: Nope, I'll be testing it out at the end of the week/next week.
And I paid significantly less than that.
I won't be working with any stains for a bit, however.
Maybe next month some point.
Wow, I can't wait! And WOW, WOW, WOW about the price!
Don't stress about the stains, you and your new partner need a little time to get to know one another!
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
I am finding some interesting objects in the blood of a family member and would like some help in discerning what they could be. This person is chronic and has much trouble with their legs. Such trouble as pain, and difficulty walking at times.
The objects I am seeing are on/in RBCs, in the WBCs (especially the lymphocytes), and free in the plasma.
I am privy to the possibility that I am actually seeing two different pathogens in the same sample.
An important question I have is this: do Rickettsia bacteria infect WBCs, particularly lymphocytes? I am finding little info regarding this question. I have learned that mycoplasmas infect WBCs, but not sure about rickettsias.
Both mycoplasmas and rickettsias infect RBCs, so I am not sure if what I am seeing are one or the other, or both.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
Of note: both mycoplasmas and rickettsias stain well with giemsa.
This last picture has a lot of stain precipitate. What I'm looking at on this pic are the organisms on the RBC that "give off" a "cloudy tail" (like in the previous two pics).
[ 07-26-2016, 01:44 PM: Message edited by: TNT ]
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
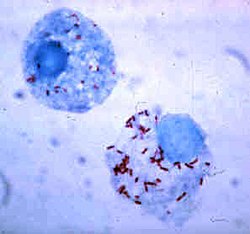
Light microscopy image of an archived Giemsa-stained blood smear from the owl monkey taken under high magnification (×1000, oil). Early trophozoites of Plasmodium falciparum (arrow heads) can be seen within the erythrocytes whilst haemoplasma bodies (arrows) can be seen on the cell membrane of the erythrocytes.
Numerous small, basophilic, Mycoplasma organisms (black arrows) on the periphery of RBCs and free in the background; a single Howell-Jolly body (arrowhead) is also present, which is much larger and more basophilic than Mycoplasma organisms. Note the single polychromatophil (white arrow) and ghost cell. Wright-Giemsa stain; magnification, 1000×.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
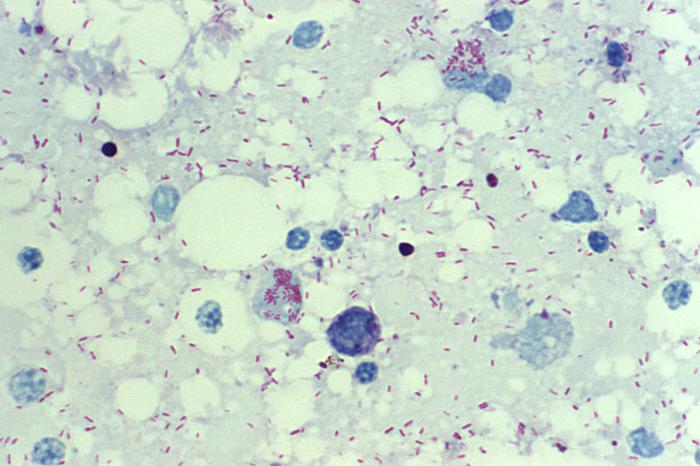
Family Rickettsiaceae was comprised of Rickettsia sp., Coxiella burnetii, Ehrlichia sp. and Bartonella sp. At one time they were thought to be viruses or a new life form. However, they proved to be bacteria that are mostly obligate intracellular parasites. They have typical Gram negative cell envelopes, 70s ribosomes and are sensitive to antibiotics. They take the Gram stain very poorly, so a Gimenez, Giemsa or Macchiavello stain is used.
Cell culture cytospin preparations stained with Diff-Quik. Top row shows rickettsiae (tip of arrows) from “Ca. R. andeanae” infected (a) A. maculatum embryonic cells, (b) ISE6 cells, and (c) Vero cells at days 47 (A. maculatum cells), 196 (ISE6), and 83 (Vero). Bottom row represents uninfected (d) A. maculatum embryonic cells, (e) ISE6 cells, and (f) Vero cells at day 196. Magnification 1,000× under oil immersion. Scale bar is equivalent to 5 μm. Images were captured by using an Olympus BX41 compound microscope and Nikon DS-Fi1 5-Megapixel CCD Color Camera. (Online figure in color.)
This photomicrograph of a Gimenez-stained yolk sac smear revealed the presence of Rickettsia rickettsii bacteria, which are the cause of Rocky Mountain spotted fever (RMSF). These bacteria range in size from 0.2 x 0.5 micrometers to 0.3 x 2.0 micrometers. They are difficult to see in tissues by using routine histologic stains, and generally require the use of special staining methods, such as the Gimenez stain used in this case.
In the human body, rickettsiae live and multiply primarily within cells that line small- to medium-sized blood vessels. Spotted fever group rickettsiae can grow in the cytoplasm or in the nucleus of the host cell. Once inside the host the rickettsiae multiply, resulting in damage and death to these cells. This causes blood to leak through tiny holes in vessel walls into adjacent tissues. This process causes the rash that is traditionally associated with Rocky Mountain spotted fever, and also causes damage to organs and tissues.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
I recently obtained an oil darkfield condenser, so some interesting pics and videos will be forthcoming! I like darkfield more than I thought I would!
There are some things I can see with darkfield that were not obvious with phase contrast. I would like to do a side-by-side comparison sometime concerning what can be seen best with darkfield vs. phase contrast. There are definite advantages with each technique.
Guys, let me know if you have any input about the preceding posts concerning the above-mentioned questions and pics.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
bluelyme
Frequent Contributor (1K+ posts)
Member # 47170
posted
Thanks tnt..in the first pics it looks like the t cells are also infected ..was that myco or rickettsia?
i am stoked for you and dude ..get us pics vids asap ..how is bvt in conjuction going? Any gains ?
-------------------- Blue Posts: 1539 | From southwest | Registered: Dec 2015
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
quote:Originally posted by bluelyme: Thanks tnt..in the first pics it looks like the t cells are also infected ..was that myco or rickettsia?
i am stoked for you and dude ..get us pics vids asap ..how is bvt in conjuction going? Any gains ?
Yes, the T-cells are infected. So far I've learned that mycoplasma can infect WBCs, but have not found info that rickettsias do. I'm hoping someone might have some further info about that.
BVT is definitely helping. If I go too long without it I start to regress. Last week I went 5 days without and got to feeling worse. The fifth day (when I stung), I felt so much better.
But, it seems I feel worse the day(s) immediately afterwards now. Stung yesterday-and felt fairly decent-but didn't sleep well last night, and today I am feeling worse with sound sensitivity, burning neuropathy (is worse), and raw nerves such that I feel "funny-bone" jolts when I bump my arms and hands.
I am convinced that BVT hits biofilms and apicomplexans *more than* borrelia & Bart-like organisms.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
Are the string of pearl forms and dumbbell looking ones considered cysts or not?
I'm trying to figure out if conventional antibiotics have any activity against these forms. Or, if they're considered cystic forms, then they would require different antibiotics.
I don't really know the physical difference between the 2 forms, or why some antibiotics work on one but not the other, so I'm just curious as to which form these "in-between" forms fall under?
Posts: 71 | From Canada | Registered: May 2016
| IP: Logged |
Lymedin2010
Frequent Contributor (1K+ posts)
Member # 34322
posted
The larger rings remind me of Theileria that infect cattle.
I will repost your pics & see if we can get outside opinion.
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
quote:Originally posted by Lymedin2010: The larger rings remind me of Theileria that infect cattle.
No, I'm not referring to the stain precipitate that looks like Theileria, I'm referring to the small bacteria.
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
TNT
Frequent Contributor (1K+ posts)
Member # 42349
posted
i.e.: In these pics, I'm referring to what appear to be bacteria inside the lymphocytes, not the stain precipitate (that looks like Theileria).
Posts: 1308 | From Eastern USA | Registered: Oct 2013
| IP: Logged |
The Lyme Disease Network is a non-profit organization funded by individual donations. If you would like to support the Network and the LymeNet system of Web services, please send your donations to:
The
Lyme Disease Network of New Jersey 907 Pebble Creek Court,
Pennington,
NJ08534USA http://www.lymenet.org/









 UBBFriend: Email this page to someone!
UBBFriend: Email this page to someone!










































 Printer-friendly view of this topic
Printer-friendly view of this topic